
Bioethics

End-of-life decisions often bring up big, complex questions—and that’s where bioethics come in. This section explores the moral and ethical issues surrounding topics like aid in dying, medical costs, organ transplantation, stem cell research, and more. With clear explanations of key principles and real-world considerations, these articles can help you better understand the tough choices people face and the values that guide them during life’s final chapter.
Jump ahead to these answers:
- What Is Bioethics?
- How Has Stem Cell Research Benefited Humanity?
- What Is Stem Cell Research and Why Is It Ethically Controversial?
- What Are the Ethical Issues Around MAID for Those Who Are Mentally Ill?
- What Is VSED and Why Is It Controversial?
- What Is the Difference Between MAID and Euthanasia?
- What Are the Ethical Arguments Surrounding Medical Aid in Dying?
- Are There Ethical Ways to Make More Organs Available for Transplant?
- What Are the Ethics Involved in Donation After Circulatory-Determined Death?
- What Are the Ethical Issues Involved in Organ Transplantation?
- What Is Age-Based Healthcare Rationing?
- How Does Cost Impact Care at the End of Life?
- What Are the Ethical Issues Around Placebo-Controlled Trials for Terminally Ill Patients?
- What Are Three Common Ethical Issues That Arise at the End of Life?
- What Is “Futile Care” and Why Is Futility an Important Consideration at the End of Life?
- Do Advance Directives Promote More Ethical End-of-Life Care?
- What Is Ethical End-of-Life Care?
- What Is a Bioethicist?
- What Is an Ethics Committee?
- What Is an Ethics Consult and How Can I Request One?
- What Is Informed Consent?
- What Is the Ethical Principle of Justice in Medical and Health Care?
- What Is the Ethical Principle of Non-Maleficence
- What Is the Meaning of Beneficence in Medical Ethics?
- What Is Autonomous Decision-Making?
- What Is the Principle of Autonomy in Medical Ethics?
- Bioethics: Additional Resources
What Is Bioethics?
July 9th, 2025According to the Center for Ethics and the Humanities in the Life Sciences at Michigan State University, bioethics is “a shared, reflective examination of the ethical issues in healthcare, health science and health policy.” Although ethical standards have always existed in healthcare and medicine, the field of bioethics seeks to integrate our traditional understanding of what constitutes “good” care and “good science” with the issues introduced by advances in medicine and technology that have taken place over the last 50 years.
Jump ahead to these answers:
The History of Bioethics
The emergence of bioethics as a formal discipline can be traced back to the mid-20th century, primarily catalyzed by breakthroughs in medical technology and research. In the 1950s and 1960s, medical advancements such as organ transplantation and the development of life-sustaining technologies, including artificial ventilation and kidney dialysis, highlighted the need for ethical guidelines in health care and health policy. These innovations raised complex questions about the definition of death, the allocation of scarce resources, and the balance between extending life and preserving its quality.
Bioethics was further shaped by the infamous Tuskegee Syphilis Study, which came to public light in the 1970s. This research, officially known as the Tuskegee Study of Untreated Syphilis in the Negro Male, was conducted by Tuskegee University in conjunction with the United States Public Health Service between 1932 and 1972. It involved 600 African-American men from Macon County, Alabama, who were told they were being treated for “bad blood.” The primary aim of the study was to observe the natural progression of untreated syphilis. However, the men were not informed about the nature of their disease nor were they given the option of treatment. Even when penicillin was recognized as an effective treatment for syphilis in the mid-1940s, it was deliberately withheld from the subjects. The study came to an end only when its details were exposed by the media, triggering public outrage and an official investigation by an Ad Hoc Advisory Panel convened by the Assistant Secretary for Health and Scientific Affairs.
That investigation, in turn, led to the establishment of the National Research Act in 1974, and the subsequent formation of the National Commission for the Protection of Human Subjects of Biomedical and Behavioral Research. Two years later, in 1976, the Commission published the Belmont Report, which established ethical principles and guidelines for research involving human subjects. These included the foundational principles or respect for persons (autonomy) beneficence, and justice. These principles continue to serve as a foundation for ethical conduct in human research today.
The rise of consumerism in the late 20th and early 21st centuries also had a profound impact on bioethics. During the early part of the 20th century, medical advances had provided physicians with an unprecedented number of innovative treatments with which to treat and cure disease. Once nearly helpless against most common illnesses and injuries, doctors were suddenly armed with a wealth of newfound knowledge, and soon came to view their authority over medical decision making as absolute. In this paternalistic landscape, the goals, values, and preferences of patients were often ignored.
During the late 1950s and early 60s, however, American consumers began to demand a greater say in decisions regarding their safety and well-being. Spurred by Ralph Nader’s scathing indictment of the automobile industry, “Unsafe at Any Speed, and the Kennedy administration’s support for consumer rights, the American public began to demand greater transparency from its institutions, and this extended to healthcare. The resulting patient rights movement focused on restoring respect and personal autonomy to individuals receiving care. As a result, several states enacted laws that required physicians to provide full disclosure on the risks and benefits associated with any proposed treatment and to obtain a signature to prove the patient understood what was disclosed. This led to the doctrine of “informed consent,” which is legally required for most medical procedures in all 50 states.
Today, bioethics plays a crucial role in guiding healthcare professionals and patients alike in making complex and morally nuanced decisions. With its focus on the ethical principles of autonomy, beneficence, and justice, bioethics ensures that medical advancements are balanced with respect for human dignity and rights. By contemplating questions surrounding medical research, end-of-life care, and reproductive technologies, bioethics provides a framework for navigating the ever-evolving landscape of healthcare with compassion and integrity.
The Scope of Bioethics
Bioethics is a complex and ever-evolving field that includes a number of different specialty areas. According to Michigan State University, some of these include:
Clinical Ethics
Clinical ethics is a practical discipline that involves resolving disagreements or conflicts in the practice of health care. More specifically, clinical ethicists help resolve conflicts that arise when patients, families, and/or healthcare surrogates and health care providers disagree about what constitutes “the best” care. For example, patients or their surrogates may decline recommended medical care or demand care that providers believe would be of little or no benefit or create suffering unnecessarily. When these types of conflicts arise, a clinical ethicist can help:
- Clarify the patient’s and family’s values
- Define and illuminate goals of care
- Promote honest, respectful communication between patients, their surrogates and the health care team
- Identify ethical issues
- Recommend a course of action that is both ethically sound and acceptable to all involved
Health Policy
Health policy ethics involve decisions made by government entities in order to manage health care as a “public good”. In a perfect world, governments would ensure that quality healthcare was accessible to all while simultaneously controlling healthcare costs. But the world is far from perfect, so ethicists in the field of health policy examine questions related to equity in health care and the dilemma of ensuring that the healthcare system is morally just. Questions that arise in this area include:
- Is quality healthcare a right or a privilege?
- Should patients be denied treatment because of an inability to pay?
- Should society’s “healthy” assume the cost of caring for those less healthy than themselves?
- Should state governments have the option of denying Medicaid to poor adults?
- How can providers assess the cost/benefit of novel treatments in a moral and ethical way?
Genetics
Now that science has succeeded in SEQUENCING THE HUMAN GENOME, genetics has taken on an ever-increasing role in healthcare. The science of genetics is used in disease prevention, the diagnosis and treatment of certain illnesses and in reproductive decisions making. Some questions that may be addressed by genetic ethicists include:
- If genetic testing shows a patient to have a hereditary, incurable disease, is that person ethically obligated to inform other family members, sacrificing their right to privacy?
- Do parents have a right to abort a fetus if a nonfatal genetic abnormality is detected in-utero? (This may also be a question for reproductive ethicists)
- How can the medical and scientific communities approach genetic testing in ways that balance individual rights with promotion of the public good?
Precision Medicine
As highly effective but extremely costly targeted therapies for cancer are becoming more and more available, the ethics of precision medicine revolve around the dilemma of when to prescribe very costly drugs that may offer limited benefit. CAR-T CELL THERAPY, for example, is a new cancer treatment that has been shown to be extremely effective in about 50% of patients treated, but for others it may extend life for only a few months. In many cases, doctors have the ability to discern, using BIOMARKERS, which patients stand to benefit the most. Since CAR-T cell treatment costs over $450,000 per patient, the question arises: As a matter of policy, should these drugs be reserved only for those who stand to benefit the most? And how should “benefit” be quantified?
Reproductive Ethics
Long an area of much debate, reproductive ethics addresses the ethical use of reproductive technologies such as in vitro fertilization, surrogacy, contraception and abortion, as well as general questions around maternal and fetal health.Some examples offered by MSU include:
- Should a pregnant woman who is brain dead be kept alive on a ventilator to ensure her fetus survives?
- Is it ethical to harvest eggs or sperm from a person after they are dead?
- Is it ethical to destroy embryos?
Neuroethics
Over the past several decades, technologies have been developed that can have a profound effect on the functioning of the human brain. Neuroethicists focus on the ethical, social and legal issues that arise as these technologies become more available and their use more widespread. For example, neurostimulation has been proposed as a therapy for a variety of conditions, from memory issues to depression. How can society ensure that these technologies are used in a sensitive, fair and ethical way?
In addition to each of these specialized areas, bioethics is concerned in general with the concept of patient autonomy and shared decision-making, a model in which the patient and provider share information and together develop a plan of care. In its purest form, shared decision-making recognizes that there are two “experts in the room” — the physician, with their years of education, learning, and medical expertise, and the patient, whose values, desires and preferences carry equal weight in a discussion about goals of care.
The Importance of Bioethics at the End of Life
Advances in medical care over the past century have drastically changed how and at what age people die. In 1900, the three leading causes of death in the United States were pneumonia, tuberculosis and diarrhea. Today, they are cancer, heart disease, and chronic lower respiratory diseases such as COPD. This shift from infectious causes of death to chronic conditions has helped to drastically improve the life-expectancy of all Americans, from 48 years in 1900 to 76.1 years in 2021.
Other medical advances have changed the landscape of healthcare and how we view the end of life. Before 1960, CPR did not exist. If a person’s heart stopped beating and/or they stopped breathing, they simply died. Mechanical ventilators, which today are widely used in hospitals to support critically ill patients, were not invented until the mid-1950s. The first intensive care units in the country also came into being around that time.
All of these technological breakthroughs add up to a new understanding of the practice of medicine and delivery of healthcare. Serious illnesses that once followed an inexorable, linear course are now much more fluid and unpredictable. People can be “dead” and then brought back to life. Life can be extended almost indefinitely with medicines, machines and expert care. And while few of us would wish to go back to a time when these options didn’t exist, these advances in healthcare have created complex bioethical questions about how, when and where people die. As Dr.Lydia Dugdale, associate professor of medicine at Columbia University, and the director of Columbia’s Center for Clinical Medical Ethics said in an interview with SevenPonds, “As any doctor or doctor-in-training will tell you, we care for many, many patients who end up lingering in the intensive care unit. From some of these patients’ perspectives, they are living a life worse than death. In some ways, the things that medicine has made possible can bring more suffering than death itself.”
Further, despite more widespread adoption of advance directives as a means of communicating end-of-life goals, these kinds of questions are rarely easy to resolve. Thus, one of the major roles of bioethicists is to help shape healthcare practices in a way that truly reduces suffering and ensures that providers honor and respect each individual’s wishes regarding how they wish to be cared for at the end of life.
Ethical Issues at the End of Life
Providing care to persons at the end of life comes with many unique challenges. People who are living in the last stages of a terminal illness suffer in numerous ways, including:
- Physical suffering due to the disease process or treatment side effects
- Loss of function (e.g. independence, enjoyable activities, satisfying relationships)
- Personal psychological factors (e.g., existential anxiety, depression, loss of a sense of purpose or meaning)
- Social and environmental factors (e.g., loss of contact with social network, availability of support)
- Spiritual factors (e.g., hopelessness, despair, fear of death or the afterlife)
Alleviating this suffering is of paramount importance to the medical team as well as to the patient and their surrogates. However, in many cases, conflicting needs and goals of care lead to ethical issues that make achieving this objective difficult. Some of the most common issues that arise include:
Communication Difficulties
Many patients cannot communicate effectively as death approaches, either due to clinical interventions (e.g.,a breathing tube); physical symptoms such as extreme weakness, confusion or shortness of breath; or the effects of symptom-relieving drugs. As a result, one-on-one communication between the patient and their care team becomes extremely difficult at a time when accurate and timely information-sharing is critical. Further, the patient’s surrogates may not be able to fully understand and process information due to the distress of watching their loved one’s suffering, whether that suffering is actual or perceived. These barriers to communication can present an ethical challenge when clinical decisions, such as whether to institute or forgo certain medical interventions, must be made.
Symptom Management
Although it is not especially common, some patients at the end of life can suffer intractable pain that is very difficult to control. Additionally, about half of dying patients will experience a phenomenon known as “terminal delirium” or “terminal agitation,” during which they become disoriented, agitated and extremely unsettled. Some patients may actively hallucinate while others will cry out, moan, or thrash about in bed. Experts believe these are not signs that the patient is in pain but rather a neurological reaction in the dying brain. Nevertheless, these symptoms can be extremely difficult for family and loved ones to watch.
In both of these scenarios, caregivers must balance the need to provide the dying patient (and their family) some measure of comfort with the risks of treating them with escalating doses of pain-killing or sedating drugs. Unfortunately, this ethical quandary often results in undertreatment of distressing symptoms and an overall poorer quality of death.
Loss of Autonomy
Similar to broken communication, loss of autonomy can occur when the patient loses the capacity to make informed decisions due to advanced illness, unconsciousness or delirium. Even in situations where an advance directive or POLST is available, lack of clarity around goals of care is not uncommon, especially if surrogate decision-makers disagree with the wishes stated in the advance directive or POLST. In these situations, the medical team is often tasked with making difficult decisions that might conflict with the patients values and goals. This situation is often exacerbated by disagreement among family members about what the best course of action should be.
Family Conflicts
Family conflicts can often arise during end-of-life care decisions, adding another layer of complexity and emotional strain to an already challenging time. These conflicts may stem from differing interpretations of the patient’s wishes, disagreements about the goals of care, or deep-seated familial tensions that resurface under stress. The high emotional stakes can create an environment ripe for discord, with family members battling over what they believe to be the best course of action for the patient. Such disagreements can pose an ethical issue for the healthcare team if the patient’s own wishes are not known.
In summary, bioethics is a complex field that attempts to address the many ethical issues that arise in today’s ever expanding healthcare landscape. It applies to decision-making in many different aspects of science and medicine, including the many fraught and confusing situations that can arise at the end of life.
Sources
“The Untreated Syphilis Study at Tuskegee Timeline”. U.S. Centers for Disease Control and Prevention. https://www.cdc.gov/tuskegee/about/timeline.html?CDC_AAref_Val=https://www.cdc.gov/tuskegee/timeline.htm
“The Belmont Report”. Office for Human Research Protections. https://www.hhs.gov/ohrp/regulations-and-policy/belmont-report/index.html
“Informed Consent”. Cleveland Clinic. https://my.clevelandclinic.org/health/articles/24268-informed-consent
“First complete sequence of a human genome”. National Institutes of Health. https://www.nih.gov/news-events/nih-research-matters/first-complete-sequence-human-genome
“CAR T Cells: Engineering Patients’ Immune Cells to Treat Their Cancers”. National Cancer Institute. https://www.cancer.gov/about-cancer/treatment/research/car-t-cells
“What are Biomarkers?”. Current Opinion in HIV and AIDS. https://pmc.ncbi.nlm.nih.gov/articles/PMC3078627/
“Life Expectancy in the U.S. Dropped for the Second Year in a Row in 2021”. U.S. Centers for Disease Control and Prevention. https://www.cdc.gov/nchs/pressroom/nchs_press_releases/2022/20220831.htm
“Critical care – where have we been and where are we going?”. BMC. https://ccforum.biomedcentral.com/articles/10.1186/cc11500
| Expert Advice: My biggest piece of advice is that healthcare directives and POLST forms need to be discussed — both with someone in the medical profession, someone you know like a nurse or a doctor, so you understand exactly what kind of care of want or don’t want, and then also with the person who is going to be making those decisions for you, your decision-maker. Talk to that person too. It’s the biggest part of communication about your preferences. Chris Wilson, RN, JD, bioethicist and patient advocate Community Healthcare Ethics.org Phone: (818) 389-8512 Email: chris@elderethics.net |
How Has Stem Cell Research Benefited Humanity?
July 7th, 2025Stem cell research has resulted in significant advancements to medicine, from its first inception with bone marrow transplants in the 1960s to more rapid progress within the last couple of decades. Stem cells are capable of developing into different types of cells, allowing them to be used to treat a wide range of diseases and disorders. Studying how stem cells mature into bone, nerves, heart muscle, organs, and other tissues can also help researchers learn about how disease develops.
In regenerative medicine, stem cells can be used to replace or repair damaged tissue and organs, which is revolutionary in the treatment of various cancers. Stem cell research has also shown promise in treating conditions like Parkinson’s, heart disease, diabetes, stroke, spinal cord injury, blindness, autoimmune disease, and more. Research is also underway to better understand how stem cells can be used in tissue engineering and 3D bioprinting of organs — advancements on this front would greatly relieve the heavily burdened organ transplant system.
Stem cell therapy and cancer
Using stem cells to treat certain types of cancer, doctors can mitigate the risk of the cell-damaging side effects associated with chemotherapy and radiation, and in certain cases, treat cancer cells directly. The stem cells used for transplants come from bone marrow (either the patient’s or someone else’s), the bloodstream (the patient’s or someone else’s), or the umbilical cord of a newborn.
Many cancers start in bone marrow or spread to it, including leukemia, lymphoma, and multiple myeloma. Stem cell therapy for cancer replaces a patient’s own stem cells that have been destroyed or damaged by cancer, radiation, or chemo. By transplanting healthy stem cells, a medical team can use much greater doses of chemo to attack the cancer, as the healthy cells will continue normal growth and reproduce cancer-free cells.
Another type of cancer-treating stem cell therapy is known as the “graft-versus-cancer” effect, which uses stem cells transplanted from someone other than the patient. Donated cells are usually more able to seek and kill cancerous cells than the patient’s own immune cells. The “graft,” aka donated stem cells, helps destroy cancer cells along with encouraging the growth of normal cells in bone marrow.
Sources
“How Stem Cell and Bone Marrow Transplants Are Used to Treat Cancer”. American Cancer Society. https://www.cancer.org/cancer/managing-cancer/treatment-types/stem-cell-transplant/why-stem-cell-transplants-are-used.html
“Regenerative Medicine”. Association for the Advancement of Blood & Biotherapies. https://www.aabb.org/news-resources/resources/cellular-therapies/facts-about-cellular-therapies/regenerative-medicine
“Introduction to Stem Cells”. National Institutes of Health. https://stemcells.nih.gov/info/basics
“Stem Cells”. What is Biotechnology? https://www.whatisbiotechnology.org/index.php/science/summary/stem/stem-cells-repair-tissues-and-regenerate-cells
“Stem Cells: What they are and what they do”. Mayo Clinic. https://www.mayoclinic.org/tests-procedures/bone-marrow-transplant/in-depth/stem-cells/art-20048117
What Is Stem Cell Research and Why Is It Ethically Controversial?
July 7th, 2025Embryonic stem cells (also known as pluripotent stem cells) are immature, undifferentiated human cells that have the capacity to develop into almost any type of cell (e.g. nerve cell, bone marrow cell, pancreas cell, muscle cell). They also have the unique ability to reproduce almost indefinitely, even after long periods of inactivity, both in the body and in the lab.
According to the National Institutes of Health, one of the main goals of stem cell research is to study how undifferentiated embryonic stem cells differentiate into cells that form tissues and organs. Understanding this process is key to finding the answers to many different diseases, including those caused by errors in cell division, such as cancer.
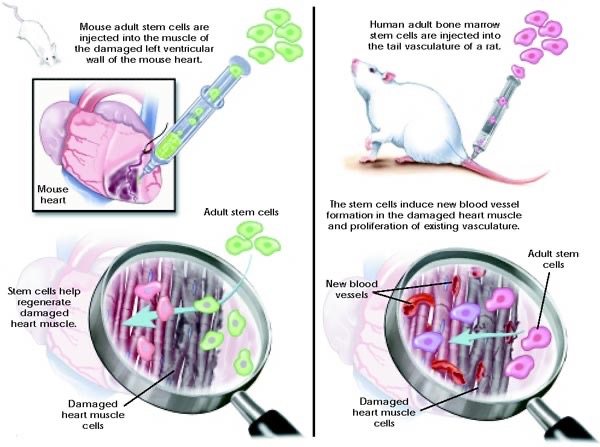
Another goal of stem cell research is to develop cell-based therapies, in which stem cells are induced to develop into a specific kind of cell. The stem cells are then injected into an ailing organ (such as a damaged spinal cord or failing heart) to stimulate the growth of healthy cells. These types of therapies have the potential to treat and possibly cure many different conditions, including diabetes, heart disease, macular degeneration, spinal cord injuries, burns, arthritis, and ALS, to name just a few. (See graphic below)
The main ethical dilemma surrounding stem cell research is the fact that the pluripotent stem cells are derived from human embryos, which are destroyed in the process of extracting the cells. These embryos are extraordinarily immature, 100-cell blastocysts that are typically about 3-4 days old. They have no neural tissue, that is, no spinal cord or brain (these do not develop until the embryo is 14 days old). Nevertheless, some opponents of stem cell research believe that, because they could develop into a fetus if implanted in a uterus, destroying them is tantamount to destroying a human life.
Since its inception in the 1990s, embryonic stem cell research has been the subject of a great deal of legal wrangling, legislation, and policy-making by the Executive Branch. However, after years of steady controversy, in 2013, the legality of stem cell research was decided by the Supreme Court. In a landmark decision, the court ruled that a 1995 law prohibiting the use of federal funds for research that involves the creation or destruction of human embryos (the Wicker-Dickey Amendment) does not apply to research performed using stem cells harvested by private institutions and later obtained by the NIH or its grantees.
Sources
“Introduction to Stem Cells.” National Institutes of Health. https://stemcells.nih.gov/info/basics
“Stem Cell Policy Timeline”. Research America. https://www.researchamerica.org/wp-content/uploads/2023/02/U.S.-Stem-Cell-Policy-Timeline-Through-2020.png
{kind=link}
“Supreme Court allows federal stem cell research to continue”. https://www.cnn.com/2013/01/07/justice/stem-cell-appeal/index.html
What Are the Ethical Issues Around MAID for Those Who Are Mentally Ill?
July 7th, 2025Ethical issues surrounding Medical Assistance in Dying (MAID) typically center around the principles of autonomy, beneficence, justice, and non-maleficence. Although MAID is legal in certain jurisdictions within the United States, it remains a topic of debate, particularly regarding its potential impact on individuals with mental illnesses. In jurisdictions such as Canada, MAID has been approved for patients with mental illness, but its implementation is currently delayed until March 2024 to allow for the development of practice standards and appropriate training. Since the practice of MAID largely depends on the patient’s legal capacity to make an informed choice, it has prompted numerous ethical dilemmas, some of which are discussed here.
Autonomy is generally defined as an individual’s ability to make decisions that will affect their lives, including decisions regarding their care. In the context of autonomy, if a patient with a mental illness has the capacity and competence to make an informed decision regarding their care, they can request that their physician evaluate their suitability for MAID. It can be argued, however, that some patients may experience impaired judgment or decision-making due to the symptoms of their mental illness, raising questions about their mental competence. Some studies have found that although depression can influence decision-making capacity, it does not necessarily reflect patient incompetence. As many as 75% of patients with mental illnesses may possess the capacity to make their own healthcare decisions.
Mental illnesses can be episodic in nature, which means that symptoms can improve over time if the patient receives suitable treatment. Symptoms can also worsen if the patient is exposed to traumatic experiences, stress, or other triggering factors. The principles of non-maleficence and beneficence, which address the duty to do no harm and to promote good, can be viewed as conflicting positions when considering patients who have requested MAID. If there is a chance that the patient’s mental status could improve with treatment, consenting to provide MAID could violate these principles since the practice affirms the patient’s decision to die. Another ethical consideration is that denying the patient’s request for MAID can be harmful if the patient genuinely believes that this is the only way to relieve their suffering.
Another ethical dilemma can arise when considering the principle of justice, which emphasizes the importance of equality and fairness to all people. In the context of MAID, justice could mean that if MAID is accessible to patients who are terminally ill, the decision to withhold MAID from patients with treatment-resistant mental illness would be unjust. Conversely, some have argued that approving MAID for patients with mental illness might inadvertently perpetuate the misconception that mental illness cannot be effectively treated. Given the wide variety of ethical dilemmas surrounding MAID, debate among patients, policymakers, and caregivers will only continue as the landscape of this practice continues to evolve.
Sources
“Your Questions on MAiD and Mental Illness”. CAMH. https://www.camh.ca/en/camh-news-and-stories/maid-and-mental-illness-faqs
“Suffering is not enough: Assisted dying for people with mental illness”. Bioethics. https://pmc.ncbi.nlm.nih.gov/articles/PMC9306695/
“Medical Assistance in Dying Should Not Exclude Mental Illness”. New York Times. https://www.nytimes.com/2023/04/21/opinion/medical-assistance-dying-mental-illness-maid.html
“Medical Assistance in Dying: Challenges for Psychiatry”. Frontiers in Psychiatry. https://pmc.ncbi.nlm.nih.gov/articles/PMC6295549/
What Is VSED and Why Is It Controversial?
July 7th, 2025VSED is an acronym for voluntarily stopping eating and drinking as a means of hastening one’s death. It is most often chosen by persons who are terminally ill and experiencing increasing suffering but who do not qualify for medical aid in dying either because they are expected to live beyond the requisite 6 months or because they live in a state where medical aid in dying is prohibited by law. In some instances, an elderly person may choose VSED because they are simply “done” with living and are ready to die.
Proponents of VSED cite it as a compassionate, relatively painless means to end one’s life, and for many people who choose the option, this is true. Depending on the person’s physical health, level of commitment and the amount of support available, the process can take as few as several days or as long as several weeks to complete. According to Compassion & Choices, the factors that most often impact the length of time it takes a person to die in this way include their:
- Age
- Underlying illness
- Physical condition, including nutritional and hydration status
- Kidney function
- Ability to avoid all fluids, even ice chips
- Readiness to die
During VSED, the person undergoing the process usually needs a significant amount of support to maintain their fast. Hospice or a physician who is willing to provide symptom management are often, but not always required. Some people will require medications to alleviate anxiety or restlessness that comes from extreme thirst. Others can manage their discomfort with distractions such as reading, engaging with friends and family, or in spiritual pursuits. Again, the amount of time it takes for the person to succumb to starvation and dehydration varies greatly. Some people become unconscious in a matter of days while others remain alert and, in some cases uncomfortable for a considerable period of time. The latter scenario can be quite difficult for family members and caregivers, so it’s important to have adequate supports in place
It should be noted here that because VSED is voluntary, it does not require a doctor’s order and is completely legal in every state. Nevertheless, if you are contemplating VSED you may wish to spell out your wishes in your advance directive and, of course, let your health care proxy know what you plan to do. Additionally, you may create an advance directive that specifies that you do not want “assisted feeding” if you develop dementia and are unable to take in food on your own. These “dementia directives” are somewhat controversial, however. Those who oppose them argue that a person with capacity cannot impose that decision on their future self, who, despite being incapacitated, may very well wish to continue to eat and drink. For this reason, they are not legal in every state and, practically speaking, are often ignored.
Another ethical objection to VSED that has been raised by some is that it is tantamount to suicide, which an ethical society cannot support. However, this objection is generally considered unsustainable by the bioethics community, since in the vast majority of cases the person choosing VSED is already dying. They are simply taking control of the timing and manner of their death.
Sources
“Washington Post Boosts Suicide by Self-Starvation”. National Review. https://www.nationalreview.com/corner/washington-post-boosts-suicide-by-self-starvation/
What Is the Difference Between MAID and Euthanasia?
July 7th, 2025Patients who opt for Medical Aid in Dying (MAID) are provided with specific prescription medications that will be self-administered when the patient is ready to die, whereas euthanasia is differentiated by these medications being administered by a physician or healthcare staff. Euthanasia is illegal in the United States, and as of 2023, MAID is currently legal in 11 states and continues to receive advocacy in states where access is restricted. Another distinguishing factor is that there is only one type of MAID, but there are many different types of euthanasia and practices that are categorized as euthanasia.
It is important to understand that the decision to withhold or withdraw life-sustaining interventions is not the same as euthanasia or MAID. Deciding to stop treatment is a common occurrence in healthcare, but the element of life-sustaining interventions is often unique to emergencies or end-of-life care scenarios. If the intervention no longer benefits the patient, doesn’t improve the patient’s quality of life, or no longer meets care goals, it is deemed appropriate to withdraw. If the patient has decision-making capacity, understands the outcome of their decision, and states that they no longer wish to receive the intervention, this also justifies the decision to withdraw. However, if the patient doesn’t have decision-making capacity, the decision may be made according to indications in an advance directive or transitioned to the patient’s surrogate in the absence of these documents.
In contrast, specific criteria must be met to be eligible for MAID. Individuals must be at least 18 years of age or older, terminally ill with a prognosis of six months or less to live, have the capacity to make their own healthcare decisions and have the ability to self-administer the prescribed medication. If someone does not meet all four of these criteria, they are deemed ineligible and exceptions cannot be made. Since euthanasia is illegal in the United States, criteria are not used to determine eligibility, but rather to discern whether a patient’s death resulted from an illegal practice rather than natural causes. In other countries, euthanasia is only legal if physicians have fully adhered to the laws pertaining to the termination of life within the region.
MAID and euthanasia differ fundamentally in method, legality, and the level of involvement between the patient and the physician. Despite these differences, most people become interested in MAID or euthanasia for similar reasons. Many people fear the dying process and have concerns surrounding reduced quality of life, poor pain management, loss of bodily function, or lack of dignity as they become more reliant on others for care. Some individuals request MAID or euthanasia because it provides them with a sense of control regarding when and how they will die. Rationale varies based on each person’s values, preferences, and concerns pertaining to the end of life.
As the societal conversation around end-of-life care continues to evolve, it’s crucial to understand the differences regarding MAID, euthanasia, and their implications in order to maintain informed and respectful discussions about these deeply personal decisions. Legislation and policies pertaining to MAID will continue to change as advocacy and the landscape surrounding end-of-life care continue to evolve and shift with the healthcare sector. Maintaining awareness of these changes and engaging in more open dialogues to reduce stigma can have a significant role in ensuring that patients with these wishes are understood, respected, and acknowledged appropriately.
Sources
“Reasons for requesting medical assistance in dying”. Canadian Family Physician. https://pmc.ncbi.nlm.nih.gov/articles/PMC6135145/
“Medical Aid in Dying”. Compassion & Choices. https://compassionandchoices.org/our-issues/medical-aid-in-dying/
What Are the Ethical Arguments Surrounding Medical Aid in Dying?
July 7th, 2025Medical aid in dying or physician-assisted death is one of the most fervently debated topics in healthcare today. Although most Americans believe that physicians should have the right to help mentally competent, terminally ill adults end their lives, many religious groups and health care professionals are vehemently opposed. Nevertheless, as of this writing, nine states and the District of Columbia have legalized the practice either through legislation or the courts.
The ethical debate over medical aid in dying is, for the most part, divided between those who support the practice and those who oppose it on religious, moral or ethical grounds.
Ethical Arguments in Support of MAID
Those who support the practice of medical aid in dying do so based on the concepts of autonomy, justice, compassion, individual liberty, and honesty and transparency.
Specifically, they include:
- Respect for autonomy: Competent human beings ought to have the right to decide when and under what circumstances they die.
- Justice: Justice requires that we “treat all cases alike.” A person who is terminally ill has the right to refuse life-prolonging treatments, such as mechanical ventilation or dialysis. So, in cases where a terminally ill person is experiencing unbearable suffering but does not require life-saving treatments to prolong life, helping them end their lives is a just act.
- Compassion: Suffering is much more than physical pain. A person may experience horrible suffering due to loss of independence, mobility, control of bodily functions and personal dignity. Sometimes, even the most compassionate care cannot relieve this kind of suffering. In that case, medical aid in dying is the most compassionate act.
- Honesty and transparency: By legalizing and legitimizing medical aid in dying, society encourages open and honest communication between patients and their doctors about end-of-life goals. This may ultimately lead to more compassionate end-of-life care.
- Individual liberty: Although society has an interest in preserving and protecting life, that interest becomes less compelling when a person is terminally ill and wants to choose when and how they die. In these cases, personal liberty rightfully ought to supersede state interest.
Ethical Arguments Against MAID
Many of those who object to medical aid in dying do so on moral or religious grounds. Others believe that allowing medical aid in dying is a “slippery slope” that puts vulnerable populations at risk. For physicians, objections may rest on professional integrity and the concept of “do no harm.”
Specifically, some arguments against medical aid in dying include;
- Sanctity of life: Historically, both religious and secular traditions hold that life is sacred and that deliberately taking a life, even one’s own, is morally wrong.
- Passive versus active: Although most people agree that withholding life-saving treatment is ethically defensible when a person is terminally ill, it can be argued that withholding treatment and allowing a person to die is not the same as actively helping a person to die.
- Potential for abuse: Some believe that legitimizing medical aid in dying puts vulnerable populations, such as the poor, the disabled and the elderly, at risk of being pressured to end their lives either to ease the burden on caregivers or to cut costs. (Note: In Oregon, where medical aid in dying has been legal for 20 years, neither of these scenarios has come to pass.)
- Professional integrity: The Hippocratic Oath, which many (but not all) medical school graduates take upon becoming a doctor, says in part, “I will not administer poison to anyone where asked,” and I will “be of benefit, or at least do no harm.” Many physicians believe this is a proscription against assisting a patient in ending their lives. What’s more, even physicians who support medical aid in dying in theory have expressed reservations about participating in the practice themselves.
- Fallibility: This argument contends that no physician is infallible, and prognoses are often wrong. Lapses in medical care can also occur, which, if rectified, might significantly improve a person’s quality of life. Doctors may also miss a diagnosis of depression in a terminally ill person who wants to end their life.
Sources
“Assemblymember & NY Alliance for Medical Aid in Dying Question Medical Society of State of New York “Survey”. Compassion & Choices. https://compassionandchoices.org/news/assemblymember-ny-alliance-medical-aid-dying-question-medical-society-state-new-york-survey/
Are There Ethical Ways to Make More Organs Available for Transplant?
July 7th, 2025The issue of how to increase the supply of available organs for transplant has received a great deal of consideration by health care professionals and policymakers in recent years. In an article titled “The Bioethics of Organ Transplantation”, Arthur Caplan, a Professor of Bioethics at New York University’s Langone Medical Center, examined the ethical considerations around a number of proposals under consideration. The most notable of these was the possibility of organ markets, or the sale of organs from living or deceased donors (with prior consent).
Currently illegal in the United States, providing financial incentives to those who would otherwise not donate their organs seems appealing, at first. But, according to Caplan, the ethical drawbacks, particularly the fact that poor people would be incentivized to donate organs in order to pay their bills, far outweigh the benefits of such a plan. As Caplan writes:
“…Watching your child go hungry while you lack a job and a wealthy person waves a wad of bills in your face is not exactly a scenario that inspires confidence in the valid choices that the poor would make in a market for body parts.”
Caplan also raises the possibility of making deceased organ donation the default position for all Americans, as several European countries have done. In other words, instead of filling out a form that says you choose to donate organs upon your death, the default would be that everyone’s organs are available for transplantation unless the person has specifically opted out. In countries that have already adopted this model, such as France, Belgium, Austria and Spain, donation rates are as high as 99 percent.
Another option that has recently become more feasible is xenotransplantation, or transplanting organs from non-human animals. Due to the very high probability of rejection, this option was heretofore considered far too risky and ethically fraught. But with the advent of genetic engineering, scientists can now breed animals that are more genetically similar to humans and less capable of inciting an immune response. (This was the case when doctors at the University of Maryland transplanted a genetically engineered pig heart into a human recipient who went on to live for two months.) Unfortunately, there are huge ethical questions around this approach as well.
Sources
“Bioethics of Organ Transplantation”. Cold Spring Harbor Perspectives in Medicine. https://pmc.ncbi.nlm.nih.gov/articles/PMC3935394/
“Ethical Issues of Transplanting Organs from Transgenic Animals into Human Beings”. Cell Journal Yakhteh. https://pmc.ncbi.nlm.nih.gov/articles/PMC4204195/
What Are the Ethics Involved in Donation After Circulatory-Determined Death?
July 7th, 2025Donation after circulatory determined death (DCD)is a protocol that allows doctors to retrieve organs from a person who does not meet the strict neurological criteria for brain death. In this scenario, the patient has usually suffered an injury or illness from which they will never fully recover, such as a catastrophic head injury or a massive stroke. They cannot breathe or maintain circulatory function without the aid of machines, and doctors have determined with reasonable certainty that they never will.
If a patient’s family or surrogate decision-maker agrees to donation after circulatory determined death, the potential donor is taken to the operating room (or a location very close to the operating room) and taken off life support. If breathing and heart function don’t resume within 2 to 5 minutes, the person is declared dead and the abdominal organs are removed. Typically, hearts and lungs are not harvested from patients who have donated after cardiac death because these organs are exquisitely sensitive to oxygen deprivation and are more likely to suffer irreparable damage before the transplant can occur. However, extracorporeal membrane oxygenation (ECMO) has recently been used to successfully reperfuse hearts that were removed from a DCD donor, offering hope that these organs can one day be harvested and transplanted successfully.
Despite its utility, donation after circulatory-determined death is ethically controversial.This ethical dilemma derives mainly from the 2 to 5 minute time limit, which is necessarily brief. (Organs deprived of oxygen for longer than 5 minutes will begin to die.) Opponents of the practice argue that there is a possibility that the patient might resume breathing on their own if surgery was delayed. And, in fact, some patients will breathe unassisted after life support is stopped, in which case the organ harvest does not occur.
Additionally, the accepted medical definition of “death” states that death must be irreversible. Thus, some ethicists believe that if breathing and circulatory function can be restored (through CPR and continued life support) the person cannot be declared dead.
For these reasons, some hospitals and physicians refuse to participate in donation after circulatory-determined death. Nonetheless, DCD is an accepted practice in many hospitals across the United States.
Sources
“Ethical Controversies in Organ Donation After Circulatory Death”. American Academy of Pediatrics. https://publications.aap.org/pediatrics/article/131/5/1021/31250/Ethical-Controversies-in-Organ-Donation-After?autologincheck=redirected
What Are the Ethical Issues Involved in Organ Transplantation?
July 7th, 2025Since the late 1950s, when the first successful kidney transplants from living donors were performed, organ transplantation has been a much sought-after option for millions of people who are critically ill. But because demand has always far exceeded supply, it has also created ethical dilemmas, such as the requisite rationing of available organs and the ever-present need to increase organ supply. In the late 1970s, the latter led to the expansion of the definition of death to include either irreversible cessation of all brain activity (brain death) or irreversible cessation of circulatory and respiratory functions (cardiac death). This change was codified in 1980 with the Uniform Determination of Death Act and was a factor in the development of the protocol known as Donation after Circulatory Determined Death.
Today, as organ transplantation becomes more commonplace, one of the most pressing ethical issues transplant providers face is the need to fairly and equitably distribute the limited number of organs available. According to the Organ Transplant & Procurement Network, the ethics of these decisions are based on three basic tenets: utility, justice and respect for persons, or autonomy. At the risk of oversimplifying these complex principles, below is a brief overview of what each of them means.
Utility
Utility refers to the notion that organs should be allocated where they will do the most good and the least harm. This means that “goods and harms” must be evaluated using standard measures to accurately inform public policy. The “goods” of organ transplantation include saving a life, alleviating suffering, and promoting well-being. These may be measured using algorithms that predict years of life added, graft (organ) survival, and quality-adjusted life years (how many years of good quality life the organ will provide). These “goods” are then balanced with potential harms, which include short-term morbidity (e.g., post-operative pain and disability) and long-term morbidities (e.g., side effects of immunosuppressive drugs, potential organ rejection, psychological effects). Other factors, such as the likelihood of graft survival, age, and the availability of alternative treatments may also be used in determining where an organ will go.
Justice
The principle of justice in organ transplantation refers to the need to treat all potential recipients with the same respect and concern. This means that the allocation of organs is never based on demographics such as race, gender or socioeconomic status, nor should the “social value” of an individual (e.g., their predicted contribution to society) be a factor in where an organ goes. Further, justice in a public program means that all individuals have a moral right to access its benefits. Therefore, justice may dictate that medical need is weighted more heavily than medical benefit (utility versus justice). In other words, an organ may go to the sickest patient even if a patient who is not as sick could predictably have a better outcome.
Respect for Persons
Based on the concept of autonomy or self-determination, respect for persons dictates that every person in the organ transplant process has the right to make decisions about their care. For example, providers should respect the decisions of surrogates who refuse to donate organs as well as the decision of a potential recipient to refuse an organ for any reason and the right of individuals to direct a donation to a specific recipient (directed donation). Because the concept of justice prevents using demographics to allocate an organ, OPTN does not allow directed donation to a specific demographic, such as a race or ethnic group.
Sources
“Donation & Transplantation History”. Health Resources & Services Administration. https://www.organdonor.gov/learn/history
“Determination of Death Act”. Uniform Law Commission. https://www.uniformlaws.org/committees/community-home?CommunityKey=155faf5d-03c2-4027-99ba-ee4c99019d6c
“Donation After Circulatory Death”. National Kidney Foundation. https://www.kidney.org/sites/default/files/03-60-0119_FBE_CirculatoryDeath_Bro_v5.pdf
What Is Age-Based Healthcare Rationing?
July 7th, 2025Age-based healthcare rationing is a concept that limits the allocation of medical resources based on the age of the patient population. This concept is rooted in the belief that the cost of care for older adults and the elderly is unsustainable due to the complexities of their prevalent medical conditions combined with the treatments and resources required to treat them. Preventative care is often perceived as less costly and more beneficial, whereas life-extending technology is significantly more expensive and provides less improvements to the quality of life for aging patients.
Although age-based healthcare rationing has been a topic of discussion for decades, concerns about its use became increasingly prominent during the COVID-19 pandemic. Many hospitals were directly affected by reductions in staff, resources, and intensive care beds, leading healthcare professionals to prioritize patient care according to the odds of survival. Since older adults and elderly patients are often exposed to ageism in healthcare, they may also have had limited access to some medical procedures due to the biases of their physicians. This led some patients to worry that they will not receive adequate care compared to younger patients.
Moreover, there have been ongoing concerns about society’s ability to maintain and support future healthcare needs, especially as the baby boomer generation continues to age. Some projections suggest that by 2030, there will be around 74 million people over the age of 65. Others have indicated that by 2034, older adults will outnumber children under the age of 18. As the healthcare system continues to struggle in the aftermath of the pandemic, there is renewed interest in age-based healthcare rationing concerning the costs associated with the general provision of care, lifesaving treatments, and emerging life-extending treatments.
While age-based healthcare rationing may have the potential to reduce costs attributed to these resources and extend the reach of preventative care to younger patient populations, it’s important to acknowledge that it’s a model that can create and exacerbate inequalities between age groups and sexes. Age-based healthcare rationing favors younger patients over the elderly, suggesting that access to resources should be based on age rather than each patient’s individual needs. Chronic conditions and wellness can vary greatly within age groups, so patients within older and elderly populations have their unique concerns. Similarly, since women live longer than men, they may be disproportionately affected by age-based healthcare rationing that would limit their access to life-extending care and other vital medical treatments. Therefore, careful considerations should be taken when implementing age-related policies to ensure that it does not perpetuate these disparities and potentially compromise the principles of ethical healthcare.
Sources
“How Elderly People Are Left Behind During Medical Care Rationing”. WBUR. https://www.wbur.org/hereandnow/2020/07/10/elderly-covid-19-health-care-rationing
“Is ageism creeping into your care of older adults?”. American Medical Association. https://www.ama-assn.org/delivering-care/population-care/ageism-creeping-your-care-older-adults
“Aging population to hit U.S. economy like a ‘ton of bricks’ -U.S. commerce secretary”. Reuters. https://www.reuters.com/world/us/aging-population-hit-us-economy-like-ton-bricks-us-commerce-secretary-2021-07-12/
“By 2030, All Baby Boomers Will Be Age 65 or Older”. United States Census Bureau. https://www.census.gov/library/stories/2019/12/by-2030-all-baby-boomers-will-be-age-65-or-older.html
“Why do women live longer than men?”. Our World in Data. https://ourworldindata.org/why-do-women-live-longer-than-men
How Does Cost Impact Care at the End of Life?
July 7th, 2025Although Americans are loath to discuss rationing of healthcare, the cost of intensive medical interventions at the end of life is an issue that’s hard to avoid. According to Kaiser Health News, in 2020, Medicare spending was $689 billion, which represented 12% of the federal budget and 20% of the nation’s total healthcare expenditures that year. What’s more, a large percentage of that money was spent during patients’ last six months of life.
There are several factors that are currently impacting Medicare spending, and unfortunately, they will continue to do so for many years to come. Most importantly, the American population is aging, so the number of Medicare beneficiaries is growing each year. According to Kaiser Health News, there were 63 million people enrolled in the program in 2020 (a number that includes younger people with a qualifying disability), and that number is expected to increase to 93 million over the next 40 years. Further, older Americans are living longer, albeit not necessarily healthier lives. In 2020, the percentage of people over 65 who were in their 80s and 90s was about 25%; that number is expected to increase to one-third over the next 40 years. Not surprisingly, health care spending increases exponentially as people age.
Another factor that is hugely impacting healthcare spending is the soaring cost of prescription drugs. According to the Congressional Budget Office, nationwide spending on prescription drugs increased from $30 billion in 1980 to $335 billion in 2018. Per capita spending increased from $140 to $1,073. And while that spending reflects a wider availability of many extremely beneficial drugs that have improved many lives, some experts believe these increases are unsustainable over the long term.
As of this writing, Medicare is legally barred from refusing to pay for a medically necessary treatment due to cost. However, the definition of “medically necessary” is open to interpretation by both private insurers and Medicare and Medicaid. One example: Medicare recently made the controversial decision not to pay for the very expensive and questionably effective Alzheimer’s treatment Aduhelm, which was approved by the FDA under fraught and highly questionable circumstances in June 2021. This was a highly unusual move; Medicare has paid for at least 80% of all FDA-approved drugs and devices in recent years. But as the cost of care continues to rise, it may become more and more common for insurers, including Medicare, to limit the treatments and drugs they will pay for, especially at the end of life.
Sources
“The Facts About Medicare Spending”. KFF. https://www.kff.org/interactive/the-facts-about-medicare-spending/
“Prescription Drugs: Spending, Use, and Prices”. Congressional Budget Office. https://www.cbo.gov/publication/57772
What Are the Ethical Issues Around Placebo-Controlled Trials for Terminally Ill Patients?
July 7th, 2025Placebo-controlled trials for patients with a terminal illness typically present complex ethical considerations. These trials have the potential to provide valuable data and lead to the development of new treatments, but are not without potential harm. Patients in the control group of trials (those who receive a placebo) are likely to be denied a potentially life-extending or life-saving treatment. And while they are already likely going to die from their condition, the treatment may extend their lives for some time. This may conflict with the ethical principle of beneficence.
Additionally, sometimes patients with certain terminal illnesses can access experimental drugs through expanded access or “compassionate use”. Expanded access allows patients with rare or life-threatening diseases to receive treatment with a medication not approved by the FDA, often outside a clinical trial. However, drug manufacturers involved in clinical trials may determine that providing patients with expanded access to experimental medications is unethical while trial participants are receiving a placebo. Similarly, participants in a trial may have their autonomy limited if they are required to use only the trial medication and avoid other potentially beneficial treatments.
A final consideration surrounds informed consent. Patients participating in clinical trials should fully understand that they may receive a placebo before agreeing to participate. However, patients with terminal illnesses may experience compromised decision-making capacity due to their circumstances and the symptoms of their condition. Some ethicists believe that providers should evaluate a participant’s decision-making capacity before enrolling them in a study to ensure the patients know what they are agreeing to.
Placebo-controlled trials involving terminal patients can quickly become a complicated ethical dilemma, depending on the circumstances. While these trials have significant potential to achieve the greater good through medical innovation, ensuring that core principles are maintained can be challenging. Ultimately, these studies should aim to maximize the potential advantages of clinical research while emphasizing the reduction of harm to patients who are vulnerable due to end-stage disease or a terminal prognosis.
Sources
“Placebo—To be or not to be? Are there really alternatives to placebo-controlled trials?” European Neuropsychopharmacology. https://www.sciencedirect.com/science/article/pii/S0924977X19318917
“How Patients with Terminal Illnesses Get Access to Experimental Drugs”. Brain & Life. https://www.brainandlife.org/articles/patients-terminal-illnesses-access-experimental-drugs
What Are Three Common Ethical Issues That Arise at the End of Life?
July 7th, 2025Some common ethical issues present at the end of life include compromised patient autonomy, shared decision-making, and the principle of double effect. Ethical dilemmas often arise in end-of-life scenarios where medical best practices conflict with patient or family preferences. Understanding the likelihood of these ethical issues and the principles at their foundation can help you anticipate and navigate them in the future should the need arise.
Respect for autonomy is characterized as the ability to respect the patient’s right to determine the next steps in their care and support their decision-making capability. When patient autonomy is compromised, issues can manifest in a variety of different ways. When patients have specific preferences regarding their treatment, the care team must respect the patient’s autonomy and deliver the most appropriate care without compromising that autonomy. However, ethical issues may emerge when the patient’s wishes and preferences are not acknowledged and supported by their partner, family or surrogate. Without proper documentation, such as advance directives, patient autonomy can be compromised and can have negative implications on the patient’s care.
Decision-making is integral to end-of-life care settings, but can quickly become an ethical issue when shared decision-making is used to make decisions on the patient’s behalf that are not aligned with their preferences and values. Being mindful of who is designated as a surrogate decision-maker can be crucial, especially in instances where the patient is incapacitated and unable to make decisions on their own. Ethical issues are likely to occur when faced with decisions regarding artificial nutrition and hydration, mechanical ventilation, terminal sedation, withholding or withdrawing treatments, and resuscitation.
Additionally, although actions may be taken to ease or relieve the patient’s symptoms, sometimes these can intersect with ethical concerns as well. For example, medication may be administered to manage a patient’s pain levels, but may hasten the patient’s death due to the potential to decrease respiration. This is known as a double effect; the intended effect is to decrease the patient’s pain, whereas the unintended effect results in decreasing their respiratory rate. Although the care team aims to provide appropriate pain management for the patient and minimize as much harm as possible, the patient’s family may perceive that the undesired effect of the medication causes harm. In many instances, the care team will need to discuss the moral and ethical intent of such treatments with the patient’s family or loved ones so that they understand the implications of these decisions.
Sources
“Ethical concerns in end of life care.” Milne Library. https://milnepublishing.geneseo.edu/nursingcare/chapter/ethical-concerns-in-end-of-life-care/
“Ethical considerations at the end of life care.” SAGE Open Medicine. https://pmc.ncbi.nlm.nih.gov/articles/PMC7958189/
“Ethics and palliative care: a case of patient’s autonomy”. Journal of Medical Ethics and History of Medicine. https://pmc.ncbi.nlm.nih.gov/articles/PMC10151720/
What Is “Futile Care” and Why Is Futility an Important Consideration at the End of Life?
July 7th, 2025According to the University of Minnesota’s Center for Bioethics, medically futile treatments are those that are “highly unlikely to benefit the patient” either by extending survival or enhancing quality of life. However, there is disagreement among bioethicists as to how to define “benefit” in this context and how to proceed when healthcare providers and patients or their surrogate decision makers disagree.
The issues around medical futility are complex. Ethical considerations include the lack of objective criteria for determining medical futility, which leads to reliance on the judgments of healthcare providers as to whether the care being provided is benefiting the patient or not. Some ethicists have expressed concern that vulnerable populations — the elderly, racial minorities, the disabled and economically and socially disadvantaged — will be denied access to life-saving treatments under the guise of futile care. Others worry that the high cost of life-saving treatments could lead healthcare providers to label some care as “futile” when there is a possibility that some benefit, however small, might be gained.
Complicating the issue further is the fact that few states in the U.S. have enacted laws that address medical futility. According to the American Bar Association, most states have tackled the issue by creating statutes that allow healthcare providers to refuse to provide treatment on a number of grounds. These include provisions for refusing on the basis of moral, philosophical, religious or personal beliefs, as well as refusing based on the fact that the requested care differs from the accepted standard of care. Fifteen states specifically allow providers to refuse to provide care that they believe will be medically ineffective or inappropriate. Only two states, Maryland and Texas, have outlined procedures for the resolution of disputes about medical futility between patients or their surrogates. Most states simply require that the provider attempt to transfer the patient to another physician or facility who will provide the requested care.
With that being said, many bioethicists believe that futility can be defined objectively if one considers prognosis, the possibility of recovery and the functional status of the patient. What’s more, by identifying care that is ultimately futile, providers can offer patients and their families more appropriate options, such as hospice, palliative care or a dignified, natural death.
Sources
University of Minnesota Center for Bioethics. https://health.umn.edu/
Do Advance Directives Promote More Ethical End-of-Life Care?
July 7th, 2025An advance directive is a legal document that instructs healthcare providers how you wish to be cared for if you are very ill and unable to speak for yourself. It also designates a healthcare proxy who will have the right to make decisions about your care if you can’t make them yourself. As such, it is a very important tool that helps doctors and other healthcare professionals understand what kinds of care you do and do not want if you are seriously ill. To that extent, it definitely promotes more ethical care.
With that being said, however, just having an advance directive doesn’t always ensure that a person’s wishes will be carried out. In fact, despite the growing number of seniors who have documented their wishes in an advance directive, studies show that these documents are often inaccessible or ignored. According to a 2010 study published in the Journal of Palliative Medicine, for example, fewer than half of all advance directives actually make it into patients’ charts. What’s more, electronic health records, which were first implemented in the U.S. in the 1960s and ‘70s to improve communication among healthcare providers, have not made finding these documents any easier. Although about 96% of hospitals in the U.S. have adopted EHRs, there is still no consistent location in the medical record where advance directives are stored.
Perhaps more importantly, an advance directive is a static document that may not address the patient’s wishes at the time a health crisis occurs. People typically prepare an advance directive in advance of a health crisis, believing they can predict what they will want when said crisis occurs. But people, being people, change their minds. Even a terminally ill person whose advance directive says “Do not resuscitate” may wish to avail themselves of life-saving measures to achieve a new goal (for example, attend a wedding or meet a grandchild for the first time). But in most cases, this change of heart won’t find its way into the advance directive or the EHR.
Certainly, it is far better to have an advance directive than not to have one. But the best way to ensure that your values and goals are respected when you can’t speak for yourself is to appoint a surrogate who clearly understands what you care about, what’s important to you, and how you would like to be cared for at the end of life, not just in some hypothetical future, but right now.
Sources
“Advance Directive Completion by Elderly Americans: A Decade of Change”. Journal of the American Geriatrics Society. https://agsjournals.onlinelibrary.wiley.com/doi/abs/10.1111/jgs.12736?referrer_access_token=sMwxEMkBssB1FtMSlXNer4ta6bR2k8jH0KrdpFOxC65I4FZRG-Z9LHoyRde0tFdOgZxECjzfM0WDVXTQWKvZNb5IDrNmpAXqPKEFrluSEOxTQ3IKmbY_MqFRpwtlZ-8T
“Documentation of Advance Care Planning for Community-Dwelling Elders”. Journal of Palliative Medicine. https://www.liebertpub.com/doi/abs/10.1089/jpm.2009.0341
What Is Ethical End-of-Life Care?
July 7th, 2025The care of elderly persons and those facing the end of life due to a life-limiting illness presents some unique challenges for care providers. These include but certainly aren’t limited to the need to maintain patient autonomy in the face of “broken” communication (e.g. when the patient can’t speak for themselves); the need to balance “goods and harms,” and the need to elicit goals of care and optimize quality of life.
Although every situation is unique, there are certain guiding principles that are a hallmark of ethical end-of-life care. These can be summed up as follows:
- The overarching goal of ethical end-of-life care is to provide care that is consistent with the dying person’s values, goals, and preferences in a compassionate, nonjudgmental, and respectful way.
- Communication with the patient and/or their surrogates should be honest, open, and transparent. Care providers need to communicate promptly and sensitively about changes in the patient’s condition that may impact goals of care.
- Before beginning any treatment, doctors should make every effort to elicit the patient’s wishes either through verbal discussion or an advance directive and/or POLST. When the patient cannot speak for themselves, and there is no advance directive, surrogate decision makers should be provided the information they need to make informed decisions based on their knowledge of the person’s preferences, values, and goals. These include the decision to forego treatment and pursue palliative or hospice care.
- Family members and other loved ones should be encouraged to interact with the dying person to provide emotional comfort and support.
- Care should be provided in a way that respects and honors a person’s cultural and spiritual or religious beliefs.
- End-of-life care should minimize suffering and physical discomfort to the greatest extent possible. When issues around risks and benefits arise (e.g., when escalating doses of painkillers might hasten the person’s death) care providers should seek input from all stakeholders (including the healthcare team) to determine a course of action that is in the patient’s best interests.
When ethical concerns arise that cannot be resolved with input from the patient, their surrogates, and members of the healthcare team, any stakeholder (the patient or his loved ones, a care provider or a disinterested third party) can request an ethics consult, which will allow trained intermediaries with expertise in bioethics to step in and help guide decisions about care.
Sources
“Ethics consultations”. AMA Code of Medical Ethics. https://code-medical-ethics.ama-assn.org/ethics-opinions/ethics-consultations
What Is a Bioethicist?
July 7th, 2025A bioethicist is a professional who analyzes medical decisions from ethical, moral, and social perspectives to ensure that healthcare providers and other professionals comply with best practices and ethical principles. They often examine many of the ethical questions that emerge in scientific, medical, legal, or political settings, but may also focus on broader issues in society. Bioethicists are key contributors in the research that informs and surrounds larger policies pertaining to organ transplantation, pharmaceuticals, genetic engineering, and end-of-life care.
The responsibilities of a bioethicist can vary based on their specialization and the setting where their services are provided. Some common duties of bioethicists can include:
- Communicating patient objections regarding medical procedures
- Advising on ethical decision-making and consulting for medical institutions
- Contributing to research and developing ethics training programs for healthcare professionals
- Representing the patient’s family in end-of-life care discussions
- Evaluating a patient’s capacity to make informed decisions
- Conducting medical research for upcoming treatment options and educating participants about the implications
- Educating professionals and patients about procedures such as euthanasia, stem cell research, abortion, or genetic engineering
- Combating misinformation and providing education to the public about controversial medical procedures and treatments
Bioethicists can fulfill many roles depending on their specialization and overall expertise. Some bioethicists focus on educating other professionals, students, and the general public about medical advancements or treatments about which many may be misinformed. They may also work as consultants and may serve on an ethics committee to provide additional guidance and recommendations to those who are facing ethical dilemmas. Others may choose to pursue research and focus more directly on conducting studies and publishing valuable insights. Overall, bioethicists have an essential role in navigating the ethical challenges that frequently intersect in healthcare and other crucial sciences.
Sources
“What is a bioethicist?” Indeed. https://www.indeed.com/career-advice/finding-a-job/what-is-bioethicist
What Is an Ethics Committee?
July 7th, 2025An ethics committee is an organizational body that addresses ethical dilemmas and issues within an institution, such as a hospital or nursing home. Ethics committees are multidisciplinary and typically composed of professionals such as physicians, social workers, chaplains, and many other vital contributors. These professionals provide guidance and facilitate ethical decision-making when challenges arise in clinical practice.
The responsibilities and tasks an ethics committee handles often vary based on the institution that requires its services. In settings where end-of-life care is prevalent, ethics committees review patient care issues and provide recommendations on resolving them. For example, if the healthcare provider and the surrogate or patient disagree regarding choices that are central to patient care, an ethics committee may be contacted for assistance in resolving the issue.
Ethics committees aim to help everyone reach an ethically and legally appropriate solution when faced with ethical challenges. Although they often interface directly with members of the care team in a healthcare setting, they are also available to meet with patients and their families to help address difficult decisions or answer questions. By maintaining oversight and providing guidance, ethics committees ensure that any upcoming decisions or next steps remain aligned with ethical principles. Ultimately, these committees are an essential component in maintaining ethical conduct in any healthcare setting.
Sources
“Ethics Committees in Health Care Institutions”. AMA Code of Medical Ethics. https://code-medical-ethics.ama-assn.org/ethics-opinions/ethics-committees-health-care-institutions
“Ethical Issues Surrounding End-of-Life Care: A Narrative Review”. National Library of Medicine. https://pmc.ncbi.nlm.nih.gov/articles/PMC4934577/
What Is an Ethics Consult and How Can I Request One?
July 7th, 2025An ethics consult is a specialized consultation provided by healthcare professionals to address concerns surrounding ethical dilemmas, values, and obstacles in decision-making. Ethics consults help patients, families, and other healthcare professionals make informed decisions when complex ethical issues complicate treatment goals. These consults can be requested by contacting a member of the care team, such as a healthcare provider or a social worker. Although many ethics consults occur in person, some consults can also be arranged and conducted over the phone if the healthcare facility has a dedicated ethics consultant available during regular business hours.
Ethics consultants typically have extensive expertise in addressing a variety of ethical issues in numerous settings. Common ethical issues that are addressed in ethics consultations include:
- Requesting help for identifying suitable surrogate decision-makers,
- Interpretation of advance care planning documents,
- Resolving questions surrounding end-of-life treatments and decisions,
- Providing guidance on the resolution of conflicts regarding treatment plans
- Further review of innovative treatments.
Depending on the complexity of the concern, ethics consultants may conduct extensive research to gather supporting information and provide an ethical analysis with recommendations to those who have requested the consultation. Additionally, ethics consultants typically focus on trying to understand the diverse perspectives and values of everyone involved so that they can help the group reach an agreeable resolution to the ethical concern.
When an ethics consultation is requested, participating physicians are expected to take certain actions, such as notifying the patient and their family if the request did not originate from them. They must obtain the patient’s agreement to participate in the consultation and cannot coerce or force their involvement. When recommendations are provided by an ethics consultant, the individuals involved in the consult should be aware that accepting the recommendations is not required. If physicians or healthcare professionals choose not to accept the recommendations of the consultant, they are expected to share a clear rationale regarding their decision.
Sources
“Ethics Consultation FAQ”. Center for Medical Ethics and Health Policy. https://www.bcm.edu/academic-centers/medical-ethics-and-health-policy/clinical-ethics/ethics-consultation-faq
“Clinical Ethics Consultation Service for UW Medicine”. UW Medicine Department of Bioethics and Humanities. https://depts.washington.edu/bhdept/ethics-consultation
“Ethics Consultations”. AMA Code of Medical Ethics. https://code-medical-ethics.ama-assn.org/ethics-opinions/ethics-consultations
What Is Informed Consent?
July 7th, 2025Informed consent is one of the most important tenets of quality healthcare. Based on the legal and moral concept of patient autonomy, it holds that all patients must be fully informed of the risks, benefits and alternatives to any treatment proposed by the health care team and voluntarily consent to treatment before it is instituted. Informed consent includes four related principles:
- Capacity: The patient must have the mental capacity to understand the information presented to them. This generally means that a person with advanced Alzheimer’s disease or dementia cannot give informed consent.
- Accuracy: The medical provider must present the patient or their surrogate with complete and accurate information about the risks, benefits and alternatives to the proposed test or procedure. This includes information about the likelihood or probability that the risks and benefits discussed will occur.
- Comprehension: The patient must understand the information presented to them. The provider is responsible for ensuring this is the case.
- Voluntary consent: The patient’s consent must be fully voluntary and free of coercion or duress.
Included in the concept of informed consent is the right to refuse treatment, even if that refusal may result in an outcome that the average person would consider undesirable (for example, worsening disability or death). In most cases, the medical provider will try to offer other options if the patient decides to forgo their recommendations. But they can’t override a patient’s decision except in cases in which:
- The patient is a minor
- The patient is mentally incapacitated by alcohol or other mind-altering substances or has a psychiatric illness that prevents them from understanding the information presented to them
- The patient is a threat to the community (for example, they have a highly communicable disease or need psychiatric care to prevent harm to others or themselves).
The requirement for informed consent is usually waived in the event that a person is unconscious or incapacitated and there is no surrogate available if immediate treatment is needed to save their life.
Sources
“Informed Consent”. AMA Code of Medical Ethics. https://code-medical-ethics.ama-assn.org/ethics-opinions/informed-consent
What Is the Ethical Principle of Justice in Medical and Health Care?
July 7th, 2025The ethical principle of justice typically pertains to fairness and equality. According to this principle, all individuals should have equal access to care and resources regardless of who they are. It also means that there should be equitable distribution of services, resources, and opportunities to ensure that individuals are not denied access to necessary treatment based on factors such as age, gender, race, religious affiliation, or socio-economic background. Like other ethical principles, elements of the principle of justice are evident in the general expectations outlined for healthcare professionals in the code of medical ethics.
Justice also means that healthcare professionals should treat all patients equally while avoiding prejudice or social discrimination. Patients that face similar challenges should generally have access to the same options and rights as other patients in the same situations. Healthcare providers are required to demonstrate impartial resource allocation and prioritize patients in greatest need, ensuring they obtain the necessary resources for recovery or survival.
This can also mean that healthcare professionals should address systemic inequalities that prevent access to care if they are aware that these barriers exist among the patient populations they serve.
Other examples of justice in action can be found in policies to improve healthcare systems, make insurance more widely accessible for individuals, and develop programs that will reduce health disparities among patient populations. Justice in relation to end-of-life care can also arise in ethical dilemmas regarding healthcare rationing, distribution of resources during crises, equal access to experimental treatments and practices such as medical aid in dying.
Sources
“Patient Rights and Ethics”. StatPearls. https://www.ncbi.nlm.nih.gov/books/NBK538279/
“AMA Principles of Medical Ethics”. AMA Code of Medical Ethics. https://code-medical-ethics.ama-assn.org/principles
“Ethical Principles in Patient-Centered Medical Care to Support Quality of Life in Amyotrophic Lateral Sclerosis”. Frontiers. https://www.frontiersin.org/journals/neurology/articles/10.3389/fneur.2019.00259/full
What Is the Ethical Principle of Non-Maleficence
July 7th, 2025Non-maleficence emphasizes the importance of avoiding actions that could potentially harm others. According to this ethical principle, professionals are morally obligated to reduce the risk of causing injury or harm to other people. Although non-maleficence is commonly discussed in the context of healthcare, it is a fundamental principle in many other professional fields. In healthcare settings, the principle of non-maleficence can influence providers to consider the advantages and disadvantages of potential treatments and interventions before suggesting the one that provides the most benefit to the patient.
Another consideration regarding non-maleficence is that it can mean avoiding causing harm or injury to others through acts of omission. For example, suppose a healthcare provider knows that a specific treatment can effectively address a patient’s symptoms but doesn’t offer that treatment even though it’s available. In that case, the omission of that option can cause harm. It can also be argued that if the provider upholds the ethical principle of beneficence, they will most likely also uphold the principle of non-maleficence, as both principles ultimately focus on promoting the well-being and welfare of the patient.
As mentioned, non-maleficence influences healthcare professionals when deciding on procedures, interventions, and treatments. This means that they must consider the benefits and risks of every action and choose the one that effectively reduces harm. However, non-maleficence also extends into other fields, such as law. In a legal setting, attorneys have a duty to avoid any actions that might harm the interests of their clients. Ultimately, non-maleficence is a guiding principle that encourages professionals to prioritize the safety of those entrusted to their care.
Sources
“Principles of Clinical Ethics and Their Application to Practice”. Medical Principles and Practice. https://pmc.ncbi.nlm.nih.gov/articles/PMC7923912/
“Principles of Bioethics”. UW Medicine. https://depts.washington.edu/bhdept/ethics-medicine/bioethics-topics/articles/principles-bioethics
What Is the Meaning of Beneficence in Medical Ethics?
July 7th, 2025Beneficence in medical ethics refers to the moral requirement of healthcare professionals to act in the best interest of their patients. It is one of the four key principles of modern bioethics, and involves promoting patient wellbeing within the context of their individual needs and goals. To align with the principle of beneficence, medical practitioners must balance the risks and benefits of treatments or procedures while considering their patients’ unique value systems.
Respect for autonomy, to the extent possible, plays a large role in the concept of beneficence as well. Healthcare professionals should ensure that patients are accurately informed of all available treatment options so they can make an informed decision about their care, and their decisions should be respected. When beneficence takes precedence over a patient’s autonomy, it is called paternalism, in which the patient/physician relationship is akin to that of a parent and child. Once the norm, under paternalism a doctor would make decisions for their patient based on what they believe to be in their best interest, even if it goes against the patient’s wishes and preferences. This type of decision-making has come under scrutiny due to ethical considerations about whether it is appropriate for a doctor to override a patient’s autonomy in favor of what they think is right.
In practice, beneficence requires balancing competing interests when making decisions. For example, if providing a certain treatment might cause harm to the patient, medical practitioners must consider whether the potential benefit of providing this care outweighs the risk of doing so. Healthcare professionals should strive to ensure that any risks are minimized and benefit to the patient is maximized, while taking into account their preferences and values. Beneficence calls for treatments that are appropriate, necessary and beneficial to patients, are based on the individual circumstances of each patient and are not influenced by external factors such as financial gain, physician bias or goals.
Beneficence in action
In an example from Tulane University, a patient arrives for treatment with a severely injured leg at high risk for infection. One option for treatment is amputation, which would mitigate the injury and prevent a possibly life-threatening infection. However, the complications of living without a limb are significant, so a beneficent physician would likely choose a course of treatment that retains the leg, ostensibly providing greater well-being for the patient, despite being less cut-and-dry in mitigation. Regardless of the treatment chosen in the above example, a physician adhering to beneficence would only move forward after consulting and incorporating the patient’s own preferences, values, and goals, and these would be different for every patient.
Sources
“Principles of Bioethics”. University of Washington. https://depts.washington.edu/bhdept/ethics-medicine/bioethics-topics/articles/principles-bioethics
“Principles of Clinical Ethics and Their Application to Practice”. Medical Principles and Practice. https://pmc.ncbi.nlm.nih.gov/articles/PMC7923912/
“Ethics in Health Care: Improving Patient Outcomes”. Tulane University. https://publichealth.tulane.edu/blog/ethics-in-healthcare/
What Is Autonomous Decision-Making?
July 7th, 2025The principle of autonomy in medical ethics refers to the right of each human person to make informed decisions about their care. With the widespread availability of life-saving medicines and technology, individuals today often have the ability — to a great extent, at least — to choose how and under what circumstances they will die. Further, U.S. law guarantees each of us the right to make those choices independently and to have them respected by the healthcare professionals entrusted with our care. A person with advancing cancer, for example, can choose to end curative therapy and enter hospice, even though they may die more quickly as a result of that choice. Similarly, an elderly person who has been hospitalized with pneumonia may choose not to be admitted to the ICU or allow doctors to insert a feeding tube. Conversely, patients have the right, at least in theory, to request life-saving interventions even when healthcare professionals believe they will do little, if any, long-term good. This ability to make informed choices about what treatments we receive and don’t receive is the essence of autonomy and autonomous decision-making.
The right to choose what happens to one’s own body is central to the guarantee of personal autonomy that is foundational in Western society. From a bioethical perspective, therefore, the role of healthcare providers in the decision-making process is to provide patients with the information they need to make decisions about their care. This includes accurate information about the risks, benefits and alternatives to all proposed treatment strategies (including the option to forego curative treatment in favor of comfort care.) Providers are ethically obligated to respect the patient’s wishes even when they strongly disagree.
When an individual lacks decision-making capacity (for example, if they are unconscious or too ill to understand what is being proposed) and there is no written advance directive that addresses the situation at hand, that person’s next-of-kin or designated healthcare proxy is legally and ethically empowered to make decisions about their care. This is based on the doctrine of “substituted judgment,” which assumes that a surrogate has the ability (based on prior discussions or knowledge) to act in a way that reflects the patient’s values and goals. And while a rather large body of research suggests that substituted judgment is a flawed concept that rarely achieves that goal, it remains the standard of care throughout the U.S.
Sources
“Substituted Judgment: The Limitations of Autonomy in Surrogate Decision Making”. Journal of General Internal Medicine. https://pmc.ncbi.nlm.nih.gov/articles/PMC2518005/
“Ethical Issues Surrounding End-of-Life Care: A Narrative Review”. Healthcare. https://pmc.ncbi.nlm.nih.gov/articles/PMC4934577/
“Law for Older Americans”. American Bar Association. https://www.americanbar.org/groups/public_education/resources/law_issues_for_consumers/patient_self_determination_act/
What Is the Principle of Autonomy in Medical Ethics?
July 7th, 2025Bioethics: Additional Resources
July 7th, 2025Kennedy Institute of Ethics
Founded in 1971 with the support of Rose Fitzgerald Kennedy and Joseph P. Kennedy Sr., the Kennedy Institute of Ethics is a center for practically engaged ethics at Georgetown University. With a founding interest in medical ethics, it is one of the oldest academic ethics centers in the world. The Institute sponsors research in areas such as health policy, genetic ethics, reproductive rights, death and dying and environmental justice, and is host to a world-renowned research library and a state-of-the-art Ethics Lab. The Kennedy Institute also offers a free online course, Introduction to Bioethics and publishes two journals, Kennedy Institute Ethics Journals and Theoretical Medicine and Bioethics. You can contact the Kennedy Institute at (888) 246-3849 or email them at kennedyinstitute@georgetown.edu.
The Hastings Center
Headquartered in Garrison, New York, the Hastings Center is a nonpartisan, nonprofit think tank comprised of experts from multiple disciplines, including philosophy, law, political science, health science and education. Founded by philosopher Daniel Callahan and psychoanalyst Willard Gaylin, it is the oldest independent interdisciplinary research institute of its kind worldwide. Its research publications span multiple fields of inquiry, including health, science and technology with the goal of informing public policy and public understanding of bioethics and its applications in the real world. You can read its publications, including case studies, special reports, and reports from the Bioethics Forum on the Hastings Center website at no charge. You can contact the Hastings Center at (845) 424-4040 or email them at mail@thehastingscenter.org.
Bioethics.com
Bioethics.com is a public service provided by The Center for Bioethics & Human Dignity (CBHD), a bioethics research center at Trinity International University. The website compiles articles from sources across the globe covering issues related to science and medicine, biotech, emerging technologies, end of life, genetic ethics and much more. It also offers a comprehensive list of resources, including bioethics journals and publications, bioethics centers and institutions, academic programs and certificates, and much more
NYU Langone Department of Population Health/Division of Medical Ethics
Founded by bioethicist Arthur L. Caplan in 2012, the NYU Division of Medical Ethics is part of NYU Langone’s Department of Population Health. With a concentration on medical ethics and biotechnology, the organization works to address the moral and practical issues that exist in healthcare today. such as ethical treatment of patients, access to investigational medicines, transplant ethics, end-of-life care and scarce-resource rationing. The division offers educational opportunities through a visiting scholar program, and internships for high school and college students as well as a number of public events held throughout the year.