
Organ, Tissue, & Body Donation

Organ, tissue, and whole-body donation can offer hope and healing to many, even after death. This section explores the different types of donation, who’s eligible, and the process involved. You’ll also find thoughtful discussions on ethical considerations and living donations. Whether you’re curious or ready to make decisions, these articles provide clear, compassionate information to help you understand and navigate these important choices.
Jump ahead to these answers:
- What Is Organ, Tissue, & Whole-Body Donation?
- What Happens to My Body After It Is Donated?
- Can I Register for Both Organ Donation and Whole Body Donation?
- Who Can Donate Their Body to Science?
- How Can I Donate My Whole Body to Science?
- What Is a Vascularized Composite Allograft?
- How Are Donated Tissues Used?
- What Is the Tissue Donation Process?
- Can Donor and Recipient Families Meet?
- What Is the Likelihood a Recipient Will Reject a Transplanted Organ or Tissue?
- What Can I Expect After Organ Transplant Surgery?
- Will Being an Organ or Tissue Donor Impact the Care Received at a Hospital?
- What Are Common Religious Views on Organ and Tissue Donation?
- What Are the Ethical Considerations Surrounding Organ and Tissue Donation?
- How Do OPTN and UNOS Work Together to Ensure Equity in the Transplant Process?
- Does Health Insurance Pay for Transplant Surgery?
- What Is the UNOS (United Network for Organ Sharing)?
- What Is the Organ Procurement & Transplantation Network (OPTN)?
- How Long Does It Take to Process a Donation of Organs or Tissue?
- Is It Possible to Restrict Organ Donation From Prisoners or Other Groups?
- Can Someone Change Their Organ and Tissue Donation Status After Registration?
- Does Race Matter in Organ Donations?
- How Are Transplant Recipients Matched With Donors?
- What Is the Transplant Waiting List?
- What Are the Risks in Being a Living Organ Donor?
- What Is Living Organ Donation?
- Who Pays for Organ Donation Surgery After Death?
- How Does Organ Donation After Death Work?
- What Is Donation After Cardiac Death (DCD)?
- What Is Brain Death?
- Can Someone Donate Organs and Tissues If They Have Selected Medical Aid in Dying?
- If a Family Member Needs an Organ at the Time of My Death, Can I Donate to Them Specifically?
- Can Certain Medical Conditions Prevent Someone From Becoming an Organ or Tissue Donor?
- Is Organ/Tissue Donation Possible When Someone Dies at Home?
- Who Can Donate Organs or Tissue?
- How Common Is Organ Donation?
- Is There an Age Limit to Become an Organ Donor?
- Why Should I Register as an Organ and Tissue Donor?
- Should I Tell My Loved Ones About My Decision to Donate Organs or Tissues?
- Can My Family Override My Request to Be an Organ Donor?
- Who Can Consent to Organ or Tissue Donation If I’m Not a Registered Donor?
- How Do I Register as an Organ or Tissue Donor?
- What Is the History of Organ and Tissue Donation?
- Before Death: Donating Organs or Body
- Organ, Tissue, & Whole Body Donation: Additional Resources
What Is Organ, Tissue, & Whole-Body Donation?
July 9th, 2025Organ, tissue and whole body donation are three ways in which an individual can gift their body, in whole or in part, to others after (and sometimes before) death. When you donate organs or tissue, your gift will be used to save lives and alleviate the suffering of other individuals whose organs have failed or who require life-enhancing tissue transplants. When you donate your whole body, you may give it to a medical school for education and research or to an organization that supplies bodies to facilities that conduct scientific research. The requirements and process for each type of donation are quite different, so it’s important to understand how each one works.
Jump ahead to:
- Deceased Organ Donation Explained
- Living Organ Donation Explained
- The Organ Donation Process
- Tissue Donation Explained
- Whole Body Donation Explained
- Whole Body Donation Exclusions
- Conclusion
Deceased Organ Donation Explained
Organ donation is a process whereby an individual donates one or more organs to others whose organs have failed. The vast majority of donated organs come from deceased individuals. The most commonly transplanted organs are:
- Liver
- Heart
- Lung
- Pancreas
- Kidney/pancreas
- Intestine
- Heart/lung
- Vascularized allograft transplants (VCA) – such as transplants of hands or a face.
Because organs require a steady supply of oxygen to remain viable, a deceased donor must be maintained on ventilator support until the time their organs are recovered (removed from the body). For this reason, organ donation is the rarest of all anatomical gifts. According to Organ Donor.gov, only three out of every 1,000 people die in a way that allows them to donate organs after death.
Organ donation is typically initiated by hospital staff after a person has been declared brain dead or is determined to have sustained irreversible brain damage and is unable to sustain vital functions without the aid of life-sustaining care. Importantly, all patients receive the same level of care whether they are registered organ donors or not. Once doctors determine brain death or, in some cases, circulatory death, hospital staff contacts the local Organ Procurement Organization, a non-profit that is responsible for coordinating the process from beginning to end. Staff from the OPO first check the donor registry to determine if the person was a registered donor. If they were not, they work directly with the deceased patient’s family to obtain consent. They also organize and facilitate any medically necessary testing, recovery of organs, and their delivery to the transplant hospital(s). If the person is a registered donor, the organ procurement organization shares that decision with the family and presents them with the legal Document of Gift.
As of this writing, a single organ donor can save up to eight lives by donating:
- A heart to one individual
- Two kidneys to two individuals
- Two lobes of the liver to two individuals
- Two lungs to two individuals
- A pancreas to a single individual
Living Organ Donation Explained
Living organ donation is another option that is available to healthy donors who wish to donate an organ while they are still alive. Living donors may donate one kidney, one lobe of the liver, a uterus, gestational tissue (placenta and amniotic fluid after the birth of a baby) or part of the intestine, pancreas or lung. They may also donate bone marrow. Because of the severe shortage of deceased donors, living donation is becoming more common.Today, about one-third of all kidney transplants performed in the U.S. are from living donors, and that number is increasing steadily thanks to innovative programs that match unrelated donors through a process known as paired donation.
The Organ Donation Process
Whether an organ donor is living or deceased, the process for facilitating and implementing the donation of organs is typically the same (with the exception of directed donation from a living donor). Once the donor is identified and consent obtained, the U.S. Organ Procurement and Transplantation Network (OPTN) enters information about the donor into a national database. A computer program then selects recipients for eligible organs based on:
- Physical characteristics such as size, age, and blood type
- Need — patients in urgent need of a transplant receive first priority
- Location — patients closest to the center where the organs are located receive priority
Once potential recipients are identified, the OPO in the geographic region where the transplant will take place notifies the transplant center, which then notifies the patient that an organ is available. The doctors at the transplant center will evaluate the recipient to determine if they are well enough to withstand the transplant. If so, the OPO arranges for the organs to be recovered.
The surgery to recover the donor’s organs is performed by a specialized transplant team in the operating room under sterile conditions. If the donor is brain dead, anesthesia is not typically used, although an anesthesiologist will attend the patient throughout the procedure to ensure organ function is preserved. Living organ donors are anesthetized like any other patient undergoing surgery.
After the organs are removed, they are placed in special containers and transported to the hospital(s) where the recipient or recipients are waiting. The transplant surgery usually takes several hours, after which the patient generally recovers for some time in the ICU.
Tissue Donation Explained
In biological terms, tissue is a group of cells having similar structure that function together as a unit. In the human body, there are four kinds of tissue:
- Connective tissue, which includes bone, cartilage, fat, blood and lymphatic tissue.
- Epithelial tissue, which protects the body’s organs and includes the outer layer of skin, and the lining of the intestine, respiratory tract and abdominal cavity
- Muscle tissue, which is divided into three types:
- Cardiac muscle, which forms the walls of the heart
- Skeletal muscle, which is attached to bones and is responsible for movement
- Smooth muscle, which is located in hollow organs, such as the liver, pancreas, stomach and intestines.
- Nerve tissue, which makes up the peripheral and central nervous systems, including the spinal cord and the brain.
Many different types of tissue can be used for transplantation, including tendons, ligaments, nerves, bones, heart valves, skin, veins and corneas. And because these tissues don’t rely on a steady supply of oxygenated blood to survive, they can be recovered from the body for a period of up to 24 hours after death.
Further, unlike organs, which must be transplanted within a relatively short time after they are removed (usually 4 to 6 hours for heart or lungs, 12 hours for the liver and up to 36 hours for a kidney) tissue can be recovered and then stored almost indefinitely. For this reason, tissue donation is far more common than organ donation. About 2.5 million tissue transplants from (mostly) deceased donors occur in the U.S. each year. A small number also occur from living donors, particularly skin (such as skin removed in plastic surgery), bone (following joint replacement surgery), bone marrow, umbilical cord blood and amniotic fluid. Except in very rare circumstances, corneas can only be donated by people who are dead.
Like organ donation, tissue donation is usually initiated when hospital staff notify the local OPO that someone who may be eligible to donate tissue has died. This notification can also be handled by family members if the person died at home or in a nursing home. The OPO then checks the donor registry to learn if the deceased individual was a registered donor. If they were not, they contact the family and request consent. They also facilitate the removal of donated tissues and their transfer to a facility that will prepare, store and distribute them.
After tissue donation, tissues are processed by a tissue processing organization to ensure viability and the absence of any pathogens. The steps involved include cleaning, cutting, washing the tissues, soaking them in disinfecting solution and antibiotics, culturing and packaging. According to Hartford Healthcare, up to 100 individual tissues can be processed from a single donor. These are then distributed to physicians for transplantation as suitable recipients are identified.
Whole Body Donation Explained
As the term implies, whole body donation involves donating your entire body for medical education or research. Bodies are typically donated for education and research through a whole body donation program at a university. These bodies may be dissected by medical or other health sciences students in the anatomy lab. The school may also support clinical skills training or facilitate medical and scientific research in accordance with the document of gift- the consent and authorization form used for anatomical gifts..
In addition to Whole Body Donation Programs, some organizations procure bodies for medical research and distribute them as needed to facilities in the U.S. and across the globe. Known as non-transplant anatomical donation organizations or NADOs, these private for-profit companies are not highly regulated, although a handful of states have enacted laws pertaining to their operation. This type of organization is different from an OPO, which has additional federal regulations that apply.
Whether you choose to donate your body to a medical school or an NADO, advanced registration is preferred. You can find a list of U.S. medical schools that accept anatomical donations at the website of the American Association for Anatomy. Keep in mind that it’s best to choose one close to your location, since the body must be picked up and transported to the facility soon after death.
If you wish to donate through a NADO, look for a company that is accredited by the American Association of Tissue Banks, a nonprofit that works to ensure that companies that deal in bodies and body parts engage in standardized business practices and maintain quality controls.
One consideration in whole body donation is that the program or organization that receives your body may provide for a low or no-cost final disposition. This is typically accomplished through cremation or alkaline hydrolysis, with the latter method only being used by 3 to 5 programs currently. In some instances, the family may request that the person’s ashes be returned to them, but this is not always possible. Check with the organization before you register to be sure. Additionally, you should make alternate arrangements for final disposition (such as a low-cost direct cremation) in case the organization cannot accept your body at the time of your death.
Whole Body Donation Exclusions
Regardless of where you choose to donate your body, it’s important to be aware that there are certain conditions that may preclude the institution or organization from accepting it. While it is rare,, the medical school you’ve chosen may have an adequate supply of body donors for the ensuing school term and simply not need your donation at the time you die. In other cases, your physical or medical condition may preclude your acceptance, even if you registered in advance. Some conditions that may bar your acceptance into either type of program include:
- An infectious disease (such as HIV/AIDS, hepatitis B or hepatitis C, or prion diseases)
- Extreme obesity or emaciation
- Your body has been autopsied or mutilated or is decomposed
- Your body was embalmed
Additionally, if the next of kin objects to the donation, the university or organization may opt to reject the donation rather than engage in a dispute.
Conclusion
The decision to donate organs, tissue or your entire body for medical research can have a lasting impact on countless lives. Organ and tissue donation saves and improves the lives of millions of desperate patients every year in ever-expanding ways. Registering as an organ and tissue donor is as simple as declaring your intention on your driver’s license or signing up online, but it is a choice that can leave a legacy for decades to come. Further, when you gift your body for education or research, you are not only helping to advance learning and scientific knowledge but also enhancing the lives of untold people across the globe.
Sources
“How Donation Works”. Health Resources and Services Administration. https://www.organdonor.gov/learn/process
“Organ Donation and Transplantation”. Cleveland Clinic. https://my.clevelandclinic.org/health/treatments/11750-organ-donation-and-transplantation
“Types of Donation”. Donor Alliance. https://www.donoralliance.org/understanding-donation/types-of-donation
“I Have A Living Donor Who Doesn’t Match. What Can I Do? OPTN Paired Kidney Donation Pilot Program”. UNOS. https://unos.org/wp-content/uploads/Brochure-108-Kidney-paired-donation.pdf
“Tissue Donation”. Donate Life America. https://donatelife.net/donation/organs/tissue-donation/]
What Happens to My Body After It Is Donated?
July 8th, 2025What happens to a body after whole-body donation depends upon the type of organization the donor has designated to receive it. When a body is donated to a whole body donation program at a university or medical school, it may be used for different purposes and undergo different preparation types. If it is preserved for anatomical study, the most common method is by embalming, in which a preservative solution is introduced to the arterial system. After embalming, the body is stored for a short period of time to ensure that the preservation is adequate for long-term study. Then it is assigned for use, often to a health sciences student such as those studying medicine, dentistry, nursing or physical therapy, who will study the body during anatomy training. Donated bodies may also be used unpreserved for clinical training or research, may be lightly preserved or used as skeletons. When the study period is complete, the body is typically cremated or disposed of using alkaline hydrolysis. The cremated remains, or ashes, may be buried, placed in a niche or scattered in a cemetery or at sea. In some cases, they may be returned to the family.
When a body is donated to a private company, the body may be used in many different ways. Known as non-anatomical donation organizations or NADOs, these private businesses operate in a largely unregulated industry that provides bodies and body parts to companies and institutions all over the globe. Donated bodies are typically disarticulated or recovered for body parts to fulfill requests. For example, a company developing a medical device for Parkinson’s disease might request a brain; a company that makes artificial heart valves might request a heart or a heart and lungs, or a company developing better helmets for football players might request a skull. Thus, one donated body can easily be distributed to many different locations all over the world. Some NADOs may return partial cremated remains to families for disposition upon request.
Health care researchers, medical device developers, and biotech companies rely on body donations to perfect technological advances that have the potential to benefit millions of individuals worldwide. However, it is important for anyone who is considering donating their body to science to understand what type of donation program they are registered with and what mission their donation is supporting.
Sources:
University of Minnesota Medical School: What is Whole Body Donation?: Found online at
“Anatomical Donation Program”. University of California Health. https://www.ucop.edu/uc-health/departments/anatomical-donation-program.html
“Made in America: U.S. body brokers supply world with human torsos, limbs and heads”. Reuters. https://www.reuters.com/investigates/special-report/usa-bodies-export/
Can I Register for Both Organ Donation and Whole Body Donation?
July 8th, 2025The quick answer is YES, anyone can register to be both an organ donor and whole-body donor. You can give the gift of life or an improved life for someone in need while still contributing your body to be used for scientific discovery. However, both organ donation and whole-body donation programs are mutually exclusive. This means that if you want to be a donor for both, you will need to register separately to do so.
Here are a few important things to note to make certain your wishes are fulfilled.
Everyone has the right to set their priority for their donation wishes, whether they would prefer organ and tissue donation or whole body donation. There are a number of ways to accomplish this, the easiest of which is to sign up as a donor when you obtain or renew your driver’s license. When registering for whole-body donation, you should indicate that you are also a registered organ donor. According to United Tissue Network, some organizations and universities that support research will accept a whole-body donor who has also donated an organ, tissue, bone or cornea. However, most medical schools, which need an intact body with which to train medical students, will not.
Other organizations may require an evaluation at the time of donation. For example, Mayo Clinic’s coordinators will consult with the organ donation organization to evaluate whether your whole-body donation is still acceptable after your death. If you have a desire to be a double donor, or you have already signed up to do so, you may want to contact your designated whole-body program to ensure they will accept you.
If for any reason organ or tissue donation is not feasible, your body may very likely still be eligible for whole-body donation. You can have peace of mind knowing that you have taken the extra steps to guarantee your body’s value to science in either case.
If it is your wish to donate your organs as well as your whole body, it is best that you register to do so while you are still alive. Alert your family to this decision and inform them of where you have registered for each. This can help to ensure your wishes are carried out by medical staff.
Sources
“Frequently Asked Questions”. United Tissue Network. https://unitedtissue.org/whole-body-donation/faqs/
“Making a Donation”. Mayo Clinic. https://www.mayoclinic.org/body-donation/making-donation
Who Can Donate Their Body to Science?
July 8th, 2025According to the University of California at Davis, any adult (age 18 and over) is eligible to donate their body to the whole body donation program. There is typically no upper age limit and donors do not have to be previously healthy: people with cancer, diabetes, arthritis, or heart disease are generally acceptable. People with medical devices like pacemakers or prosthesis, with surgical implants, or those with piercings and tattoos are also eligible.
However, there are a number of medical conditions that may preclude your acceptance. Some of these include:
- Hepatitis B or C
- HIV/AIDS
- Tuberculosis
- Kuru
- Creutzfeldt-Jacob’s disease
- MRSA/VRSA (Methicillin resistant and vancomycin resistant staphylococcus aureus)
- Recent extensive surgery
- Severe trauma to the body
- Extreme obesity (*Many organizations set weight limits)
- Severe muscle wasting or cachexia
Criteria for exclusion can vary, so it is important to check with the program. Bodies that have been autopsied or embalmed may be excluded as well. However, organ donation does not necessarily preclude whole-body donation, said Deanna Santana, the director of public relations at Sierra Donor Services, in an interview with SevenPonds. If you want to be an organ donor and donate your body to science, you must register separately for both and take note of important factors to ensure you qualify [link to Q/A addressing both].
Keep in mind, however, that even if your medical condition at the time of your death doesn’t exclude you, there may be other reasons why you may not be accepted into the program of your choice. For example, the medical school you chose may already have enough bodies for the number of students studying in the lab. Or the NADO may be at capacity at the time you die.
Legal or consent issues may also arise. For this reason, it’s always a good idea to have a backup plan, such as direct cremation, [link to cremation], in place so your family isn’t left to make final arrangements immediately after your death. You may register with more than one NADO to optimize your chances of acceptance, but there are legal implications to this since the most recent disposition plan you make is the one that will generally be accepted as your final wishes. Indicating your priorities in your advance directive can be helpful in this regard, especially if you do intend to have a backup plan such as direct cremation.
Remember, too, that even if you didn’t register with a whole-body donation program before your death, your next of kin may authorize donation after you die. It may be a little more logistically challenging, but most programs will work with the family to expedite the process if they can.
Sources
“Body Donation Program: Frequently Asked Questions”. UC Davis Health. https://health.ucdavis.edu/body-donation/frequently-asked-questions
“Non-transplant Anatomical Donation”. American Association of Tissue Banks. https://www.aatb.org/nados
How Can I Donate My Whole Body to Science?
July 8th, 2025If you want to donate your body for scientific research, start by contacting a nearby university medical school. Many medical schools use donated bodies for training students in the anatomy lab, for clinical skills development or for research and have a whole-body donation program on site. The American Association for Anatomy’s website offers multiple lists to direct you to participating universities in your state.
Once you have identified a university in your area with a whole-body donation program, contact them directly to review the process with the program coordinator. In most cases, you’ll be asked to fill out a registration form. When this has been reviewed and you’re accepted as a donor, the program coordinator will send you an identification card.
In addition to medical schools, some private companies accept whole bodies to be used for research and training at locations throughout the U.S.and around the world. Bodies donated to these organizations are used for many different purposes, including:
- Education
- Research
- Training
- Development of drugs or biologics
Known as non-transplant anatomical donation organizations or NADOs, these private companies are regulated in a handful of state laws in terms of how they obtain consent from the donor or their family, how they handle and transport the body of the deceased, and how tissue is distributed, since the whole body is rarely used. In other states, they are not regulated. If you wish to contract with a company that ascribes to the higher standards of the American Association of Tissue Banks, you can find a list of accredited NADOs in our available sources.
Whether you donate your body to a private NADO or a medical school, there is typically no cost to the donor or their family for transportation, tissue recovery or final disposition. Companies make their money from the organizations that receive the body or, in most cases, body parts. These may be billed as handling or processing fees.
After studies are complete and/or usable tissue removed, the body will either be cremated or disposed of via alkaline hydrolysis (link to heading on AH in alternatives to burial and cremation], each of which turns the body to “ash.” Some universities may return donor bodies to the next of kin for burial. Each organization has its own protocol as to what happens to the ashes afterwards. UCLA’s whole body donation program, for example, scatters the ashes at sea, but some organizations will return the ashes to the family upon request.
As with organ and tissue donation, you should document your plans for whole-body donation in your advance directive and inform your family of your decision. Keep your identification card with your important documents, and make sure your loved ones know who to call. Most NADOs require that donated bodies arrive at their facility within 48 hours of death.
Sources
“Human Body Donation Resources”. American Association for Anatomy. https://www.anatomy.org/ANATOMY/About-Us/What-Is-Anatomy/Body-Donation-Policy.aspx
“Accredited Tissue Bank Search”. American Association of Tissue Banks. https://www.aatb.org/accredited-bank-search
What Is a Vascularized Composite Allograft?
July 8th, 2025A vascularized composite allograft (VCA) is a multi-tissue transplant involving structures such as nerves, skin, blood vessels, bone and connective tissue. It is a complex procedure that is characterized by the transplantation of these structures as a single unit, such as a hand or face, from a deceased donor to a recipient. VCAs are often considered to be a breakthrough in transplant science since it has the potential to serve as transplants for complex body parts.
Successfully conducting a VCA requires careful planning and execution to reduce the risk of rejection. There must be a close match between the donor’s and recipient’s tissues to ensure compatibility. Additionally, the procedure involves intricate connections between nerves, blood vessels, and other tissues from the donor’s body part to the recipient’s body. Following the surgery, the recipient must take lifelong immunosuppressant medications as a preventative measure against the rejection of the transplanted tissues.
There are some unique concerns regarding VCAs in relation to end-of-life decisions and organ donation. Since the donation process involves deceased donors, ethical concerns about consent and donor wishes are inevitable. The donor’s family often has to make decisions about these donations immediately after the loss of a loved one. However, all VCAs require authorization in addition to the standard donor registration. Consent to VCA must be explicitly stated on the registration form by the donor or by a next-of-kin at the time of death. These actions ensure clarity of consent regarding VCAs and the appropriate use of donations.
Similarly, since VCAs often involve visible body parts such as a face or hands, these transplants can be emotionally charged and sensitive for donor families. It is not uncommon for families and loved ones of a donor to continue associating VCAs with the donor, even though the transplant now belongs to the recipient. In most cases, donor families are not directly informed about the identity of the recipient unless it has been specifically arranged and agreed upon before the transplant.
Sources
“Vascularized Composite Allotransplantation”. Science Direct. https://www.sciencedirect.com/topics/medicine-and-dentistry/vascularized-composite-allotransplantation
“Vascularized Composite Allotransplantation (VCA) Research”. American Society of Transplantation. https://www.myast.org/vascularized-composite-allotransplantation-vca-research
“Vascularized Composite Allografts (VCAs)”. Donate Life America. https://donatelife.net/donation/types/vca-donation/
How Are Donated Tissues Used?
July 8th, 2025Donated tissues are primarily used for tissue grafts and tissue transplants, which are becoming far more common both in the U.S. and internationally. According to the U.S. Centers for Disease Control and Prevention, about 1 million tissue grafts are performed each year in the U.S. alone. These represent about half of all tissue released. The remainder of the tissue may be stored for use at a later time or, if quality has deteriorated, destroyed.
Corneal transplants are among the most common tissue transplants, with approximately 80,000 transplants performed each year. The sclera (the white protective layer of the eye) can also be preserved and used to repair another person’s damaged sclera, nasal septum, ear drum or gums. Corneal transplants are successful about 95% of the time, and are one of the few transplants that require no tissue or blood-type match because the cornea has no blood supply.
Another common use for donated tissue are bone grafts. These are often used in hip or knee replacement surgeries, dental implants and to augment metal hardware used to repair badly broken bones. Some other common tissue transplants include:
- Skin grafts to aid the healing of burn victims and people who have had disfiguring injuries
- Tendon grafts to replace damaged tendons such as a torn anterior cruciate ligament or ACL
- Veins used in heart transplant surgeries and procedures to reroute or re-establish blood flow to damaged organs like the heart and lungs
- Heart valve replacement
Additionally, doctors are now performing vascularized allograft transplants (VCA), which is the transplantation of a composite of tissue such as skin, muscle, bone, nerves, arteries and veins. These transplants are most often performed when a person suffers a devastating, disfiguring injury in an accident such as a car crash or fire. The process can involve the transplantation of limbs, the face or one or both hands. The donor and recipient must be carefully matched for tissue and blood type, and the recipient must be on a strict regimen of immunosuppressive drugs for life. Still, the results can be life-changing. One dramatic example: In 2020, 22-year-old Joe DiMeo, underwent a face and double hand transplant at Langone NYU hospital after a devastating car wreck left him with burns over 80% of his body two years before. The transplants came from a single donor, and were the first of their kind to succeed. Today, Joe has facial features like eyelids, a nose and lips and is regaining function in his transplanted hands.
Sources
“World’s first face and hands transplant gives New Jersey man a second chance at life”. CNN. https://www.cnn.com/2021/02/03/us/face-and-double-hand-transplant/index.html
What Is the Tissue Donation Process?
July 8th, 2025Unlike organ donation, which only takes place under very limited circumstances, the tissue donation process has few limitations. The potential donor does not need to die in a hospital or a nursing home. As long as an organ procurement organization or tissue bank is promptly notified and can retrieve the body within 24 hours, almost all body tissues, including tendons, ligaments, blood vessels, bone, heart valves and corneas, can be removed and stored for use later on. However, the process will vary slightly depending on the location of the donor at the time of death.
Death in a Hospital
In the United States, the National Organ Transplant Act of 1984 mandates that hospitals report all deaths to a regional organ procurement organization or OPO. When a person dies and the OPO is notified, the transplant coordinator or a designated agent first checks with the hospital to learn if the person is a suitable organ or tissue donor based on their medical condition at the time of death. If the person meets the criteria, the OPO then checks the state and national donor registries to determine if the patient was a registered organ and tissue donor. If they are, a representative will contact the next of kin and explain the process to the family. (Families cannot override first-person consent, but are contacted before donation occurs.)
If the person who died was not a registered organ donor, an OPO representative will contact the family or designated healthcare agent to discuss donation with them. If the family consents, the rest of the process will proceed. The family will also be asked to fill out an infectious disease and behavioral screening for the deceased.
Once consent is established, the organ procurement organization will arrange for the body to be removed to a tissue bank, where all eligible tissue will be removed by a specially trained technician under sterile conditions. At that time, blood samples will also be obtained and screened for infectious diseases, including HIV, tuberculosis, hepatitis B, hepatitis C, CMV, syphilis, cytomegalovirus, (CMV) and Epstein-Barr virus (EBV).
After all tissues are harvested, the medical director of the tissue bank will review the medical records. Only tissue that is safe for transplantation (e.g. free of infectious diseases that can be transmitted to the recipient) will be released. In the meantime, all incisions are closed and the body is returned to the funeral home or family for burial or cremation. Cosmetic implants are made where necessary so the family can have an open casket viewing if they so desire.
Death at Home or in a Nursing Home
Nursing homes are not mandated by law to report a death to the regional OPO, so the process for tissue donation when a person dies at home or in a nursing home is essentially the same. The next of kin or designated healthcare agent is responsible for contacting the regional organ procurement organization and notifying them that a death has occurred. The OPO will then check the state and national donor registries to determine if the person is a registered donor. If they are, the OPO will contact a tissue bank, which will send a technician to retrieve the body so that tissue harvest can proceed. The next of kin or healthcare agent can also consent to donation at this time.
Although tissues are less dependent on a steady blood supply than organs, there is nevertheless a short window in which to notify the OPO since tissue must be harvested within 24 hours of death. The best way to facilitate this is to have the contact information for your local OPO available and to make sure you have your loved one’s donor registration information on hand. You can locate your regional OPO on OrganDonor.gov.
Sources
“How Donation Works”. Health Resources & Services Administration. https://www.organdonor.gov/learn/process
“First Person Consent: OPOS across the country are adapting to the change”. United Network for Organ Sharing. https://unos.org/wp-content/uploads/unos/registires_combined.pdf First
“About Cytomegalovirus”. Centers for Disease Control and Prevention. https://www.cdc.gov/cytomegalovirus/about/index.html
“About Epstein-Barr Virus (EBV)”. Centers for Disease Control and Prevention. https://www.cdc.gov/epstein-barr/about/index.html
“Volunteer Locally”. Health Resources & Services Administration. https://www.organdonor.gov/get-involved/volunteer
Can Donor and Recipient Families Meet?
July 8th, 2025Yes, organ donor and recipient families can meet if they both agree. The transplant hospital and organ procurement organization manage the correspondence process to maintain confidentiality. Communication between donor and recipient families typically occurs via letters or cards, which are exchanged through the transplant center to maintain anonymity. If both families are interested in communicating and eventually decide to meet, the transplant center will facilitate a meeting.
Transplant centers manage the correspondence and meeting process between families since they understand that the decision to interact and meet is often deeply personal. Some families find it comforting to communicate with the recipient of their loved one’s donation, whereas others may find it very overwhelming. Some families are comfortable expressing their gratitude in writing but are not comfortable meeting in person. Some families prefer not to communicate with each other at all. Transplant centers try to respect these differences and accommodate them as much as possible while working to maintain the privacy of donor and recipient families. Most transplant centers have their own requirements about family correspondence and meetings, but ultimately, they strive to ensure that all correspondence and interactions are achieved by mutual consent.
Donor and recipient family meetings can be emotionally charged, often provoking complex emotions of gratitude and grief. These meetings can provide a sense of connection, reassurance, or a reminder that a loved one’s donation has made a positive difference in someone’s life. However, since these meetings can create an intense mix of emotions, many transplant centers offer counseling and support before and after the meeting. It is common for families to have an initial meeting with a transplant professional to prepare before meeting with another family and to have a debrief meeting to discuss the experience afterward.
Ultimately, meetings between donor families and recipients are possible but need careful consideration. Although these interactions can provide emotional benefits, they require sensitivity to both families’ emotional readiness and privacy. Meeting is a significant personal decision based on the comfort level of the families involved and should be respected. Families considering meeting but uncertain if they are ready to take this step are highly encouraged to seek additional support and guidance from the professionals at their local transplant center.
Sources
“Connecting donor families & recipients.” United Network for Organ Sharing. https://unos.org/transplant/connecting-donors-and-recipients/
“Contacting my donor family.” United Network for Organ Sharing: UNOS Transplant Living. https://transplantliving.org/community/contacting-my-donor-family/
“National communication guidelines.” National Kidney Foundation. https://www.kidney.org/national-communication-guidelines
What Is the Likelihood a Recipient Will Reject a Transplanted Organ or Tissue?
July 8th, 2025The rejection rate for organs or tissues varies based on several factors, including:
- The type of organ or tissue transplant
- The overall effectiveness of post-transplant care
- The response from the recipient’s immune system
Three types of rejection can occur. These include:
- Hyperacute rejection
- Acute rejection
- Chronic rejection
Hyperacute rejection occurs within minutes of the transplant and is the result of a complete mismatch of antigens. If the organ or tissue is not removed immediately, the patient will die. This rejection reaction is extremely rare due to the sophisticated technology available for matching organs today.
Acute rejection occurs within the first week to three months after a transplant. All transplant recipients experience acute rejection to some extent as their body’s immune system recognizes the presence of a foreign organ. This type of acute rejection is managed with a combination of immunosuppressive medicines such as steroids and cyclosporine A. These medicines have reduced rejection rates for organ transplant recipients by 10 to 15%. Rejection of transplanted tissue is very rare.
Chronic rejection occurs over many years due to the recipient’s continued immune response to the transplanted organ or tissue. Over time, this can damage the transplanted organ, leading to decreased organ function or organ failure. There is no way to predict or prevent this type of long-term rejection, although prompt recognition of symptoms is important to maintain organ function as long as possible.
The likelihood of rejection varies based on the organ or tissue transplanted and the degree of tissue match between the donor and recipient. For example, transplants from relatives have a lower risk of rejection, and rejection rarely occurs in transplants between identical twins. Cornea transplants are also seldom rejected since the cornea doesn’t receive any blood supply from the body, so there is a low chance of an immune reaction from the recipient.
Sources
“Transplant Rejection.” MedlinePlus. https://medlineplus.gov/ency/article/000815.htm
“Preventing Organ and Tissue Rejection.” Donor Alliance. https://www.donoralliance.org/newsroom/donation-essentials/preventing-organ-and-tissue-rejection/
“Cyclosporine”. StatPearls. https://www.ncbi.nlm.nih.gov/books/NBK482450/#:
What Can I Expect After Organ Transplant Surgery?
July 8th, 2025Although successful recovery after organ transplant surgery depends upon many factors, medical advancements continue to improve outcomes in the United States. While statistics vary widely depending upon which organ was received, whether a donor is alive or deceased, age and general health of the recipient, and other factors, survival rates have steadily increased across the board. Kidneys are the most successful of all organ transplantations. Patient survival rates at one, three, five, and 10 years are 91.27%, 86.46%, 81.17%, and 78.15% respectively.
Following surgery, organ recipients can expect to remain in the hospital for about 3-5 days following a kidney transplant and up to two weeks for other organs, such as a heart or lungs. The transplant team will monitor recovery closely and provide needed supportive care. Like most surgeries, tenderness at the site of the incision is common in the first week. In most cases, patients are encouraged to start moving slowly soon after transplant surgery.
Immunosuppressive medications will be administered to lessen the chance of organ rejection. These drugs help to keep the immune system from attacking the new organ. Recipients will need to take some type of antirejection medication for the rest of their lives.
Although the benefits of receiving a new organ certainly outweigh the risks, there are a few risks associated with organ transplant surgery. These include:
- Complications related to use of anesthesia, including death
- Blood clots and bleeding
- Post-surgical site infection
- Infection: antibiotics are generally prescribed for up to 6 months to reduce risk
- Organ rejection or failure
What to expect after kidney transplant surgery
Beyond the recovery protocol and risk factors noted above for most organ transplants, kidney transplantation requires some additional care to ensure success. In most cases, the kidney makes urine right away. A catheter helps keep urine flowing properly while the patient heals.
There are specific risks associated with kidney transplantation both before and after the hospital stay. These include:
- Acute Tubular Necrosis (ATN) or Delayed Graft Function – This means your kidney may be sleepy, or slow to wake up. Levels of creatinine remain too high because the kidney is not functioning well. Dialysis may be required for several weeks to months while the kidney recovers and creatinine levels drop.
- Primary non-function – This means that the new kidney never starts working. In this case, a biopsy will be performed.. If irreparable damage is discovered, the kidney will need to be removed. A patient is put back on the waiting list; the original wait time is reinstated to increase the chance of a replacement kidney sooner than later.
- Dehydration – can cause creatinine levels to stagnate or drop, which threatens organ acceptance
- Urine Leak – During the transplant surgery, surgeons had to replace the ureter, the tube that travels from your new kidney to your bladder. This can separate from the bladder causing internal leakage. Surgery is the only treatment option to reconnect the ureter.
Recovery expectations at home for all organ recipients
After leaving the hospital, patients are required to follow a strict regimen to ensure their new organ continues to work properly. All physician orders must be followed regarding scheduled visits, lab tests, and medications. Although some daily physical activity may be advised, it is best to avoid heavy lifting, strenuous activities, or driving for the first few weeks.
The transplant team will monitor the patient’s blood 1 to 2 times a week for creatinine levels and more. Patients are expected to closely monitor their health at home, as well. Changes in blood pressure, weight, temperature, or pulse may indicate complications and should be reported.
Organ rejection is the most constant threat to the patient’s health. Anti-rejection medications may need to be adjusted over time. Organ recipients must always guard against exposure to illness, as these medications weaken the immune system. Patients are also at a higher risk of infections, so any sign of fever, drainage from the surgical site, or an illness that does not resolve itself should be reported to the medical care team.
Other medications may be given in conjunction with immunosuppressants to ease a variety of potential side effects, which may include the following:
- Acne
- Headache
- Nausea or diarrhea
- Dry mouth
- Swollen or bleeding gums
- Mouth ulcers, tumors or thrush
- Hair growth or loss
- Bone thinning or damage
- Elevated blood sugars or Diabetes
- High blood pressure
- High cholesterol
- Weight gain
If all goes according to plan, full recovery can be expected about 3 months following surgery. The probability of living a quality life after organ transplant surgery is increased by maintaining a healthy lifestyle, including a balanced diet and regular exercise.
Sources
“Graft and Patient Survival Rates in Kidney Transplantation, and Their Associated Factors: A Systematic Review and Meta-Analysis”. Iranian Journal of Public Health. https://pmc.ncbi.nlm.nih.gov/articles/PMC8643514/
“Immunosuppressants (Anti-rejection Medicines)”. National Kidney Foundation. https://www.kidney.org/kidney-topics/immunosuppressants-anti-rejection-medicines
“Acute tubular necrosis”. MedlinePlus. https://medlineplus.gov/ency/article/000512.htm
“Creatinine”. National Kidney Foundation. https://www.kidney.org/kidney-topics/creatinine
“Primary Nonfunction of Renal Allograft Secondary to Acute Oxalate Nephropathy”. Case Reports in Transplantation. https://onlinelibrary.wiley.com/doi/10.1155/2011/876906
“Early urological complications after kidney transplantation: An overview”. World Journal of Transplantation. https://pmc.ncbi.nlm.nih.gov/articles/PMC6134271/
Will Being an Organ or Tissue Donor Impact the Care Received at a Hospital?
July 8th, 2025No, choosing to be an organ or tissue donor will not impact the care you or a loved one receives at a hospital. It is a common myth that a patient’s medical care is influenced by whether they are a registered donor. This concern often prevents individuals from registering for organ and tissue donation. However, the reality is that healthcare professionals are ethically and legally responsible for providing the highest quality care to all patients they serve, regardless of the patient’s donor status. They adhere to strict ethical guidelines and codes of conduct, which mandate them to act in the patient’s best interest.
Physicians who provide care in a hospital or emergency setting differ from physicians or surgeons who perform organ recovery and transplant surgeries. Additionally, whether a patient’s organs and tissues are suitable for donation is determined after death. The medical team responsible for the patient’s care while they are alive doesn’t know whether the patient’s tissues and organs will even be appropriate for donation after death. This eliminates any potential bias or influence over the care they provide. Additionally, less than 1 percent of patients who die in a hospital meet the criteria to be organ donors. So, the probability of finding eligible or ideal donors remains rare.
Sources
“Organ Donation and Transplantation”. Cleveland Clinic. https://my.clevelandclinic.org/health/treatments/11750-organ-donation-and-transplantation
“Get the Facts: Does saying “yes” to becoming an organ donor affect the medical care I receive?” Donor Alliance. https://www.donoralliance.org/newsroom/donation-essentials/get-facts-saying-yes-becoming-organ-donor-affect-medical-care-receive/
“Why doctors WILL NOT let you die if you’re a registered organ donor”. Donate Life – Donor Network of Arizona. https://www.dnaz.org/why-doctors-will-not-let-you-die-if-youre-a-registered-organ-donor/
What Are Common Religious Views on Organ and Tissue Donation?
July 8th, 2025While views can vary among different faith traditions, many religions support organ and tissue donation to save lives since it aligns with teachings pertaining to compassion and acts of charity towards others. Most major religions in the United States support the decision to be a donor. However, individual beliefs and interpretations can vary, so it is important to be mindful that some individuals may have personal reservations or concerns about organ and tissue donation.
Christianity and its various denominations are generally not opposed to organ and tissue donation since it has the potential to save human life. This applies to denominations such as Baptist, Assembly of God, Christian Science and many others. Some denominations, such as the Disciples of Christ, also encourage the devout to pray for transplant recipients.
Organ donation is permissible within the Islamic faith, assuming that the Shariah principles are met. Living donation is acceptable if it saves the life of the recipient or maintains their bodily function. However, deceased donation is only permissible if the donor agreed before death or if their surviving relatives have agreed after death has occurred. It should be noted that Islamic scholars have not always agreed on the permissibility of organ and tissue donation, and their teachings reflect three conflicting perspectives. These perspectives include that organ donation is impermissible, organ donation is permissible if certain conditions are met according to the law, and organ donation can become permissible even if it is impermissible in principle.
Within Judaism, organ and tissue donation are generally encouraged since saving a life (Pikuach Nefesh) is viewed as the greatest mitzvah, or commandment. Due to the value of saving a life, it is also possible to override other requirements such as observing Shabbat or ensuring that the body of the person who died is buried in whole if organ or tissue donation is involved. In general, it is considered to be a morally praiseworthy act, but perspectives on permissibility can vary based on the interpretation of the law.
Ultimately, the decision to donate is often a personal choice that can be shaped and influenced by religious beliefs. Individuals who are uncertain of whether organ or tissue donation is acceptable are encouraged to consult with their religious leaders or organizations for further guidance. Since religious leaders can have conflicting views, it may also be advisable to consult with multiple leaders to gather more comprehensive insight prior to making a decision.
Sources
“Organ Donation and Religion”. Donate Life. https://donatelife.net/donation/organ-donation-and-religion/
“The Moral Status of Organ Donation and Transplantation Within Islamic Law: The Fiqh Council of North America’s Position”. Transplantation Direct. https://pmc.ncbi.nlm.nih.gov/articles/PMC7056282/
“Orthodox Judaism: Organ & Tissue Donation”. LiveOnNY. https://www.liveonny.org/orthodox-judaisms-perspective-organ-donation/
What Are the Ethical Considerations Surrounding Organ and Tissue Donation?
July 8th, 2025Some of the prominent ethical considerations about organ and tissue donation involve concerns about shortages, allocation and financial incentives. It is difficult to fully meet the demand of fulfilling transplants for individuals who have been assigned to a waitlist since there is a significantly higher demand compared to a substantially lower supply. Unique challenges often arise as policymakers, patients and other stakeholders consider potential alternatives that would make viable organs and tissues more readily available to all who need them.
In the United States, organ and tissue donation occurs with explicit consent, sometimes known as the “opt-in” system. This ethical approach respects the autonomy of all individuals by allowing them to proactively register to become a donor. Although the opt-in system upholds individual rights, it has frequently led to shortages of viable organs and tissues since potential donors don’t always register. Some critics have argued that explicit consent for donors is less effective in comparison to presumed consent, which is utilized in other countries. However, introducing presumed consent may create concerns regarding coercion.
Financial incentives aren’t currently utilized for organ and tissue donation, but some individuals have suggested that introducing them would help address the issue of organ and tissue shortages. Similar to how incentives are provided for blood and plasma donations, monetary incentives could include direct cash payments or vouchers. While this would likely increase the number of registered donors, it would also raise ethical concerns pertaining to coercing individuals from vulnerable or economically disadvantaged populations into donating for financial gain.
Another common ethical consideration surrounds organ and tissue allocation. The United Network for Organ Sharing has numerous policies that strive to emphasize medical urgency, waiting time, and the likelihood of a successful transplant when looking at the allocation process. These policies are also actively reviewed to maintain oversight of their efficacy. Despite these efforts, many individuals have consistently expressed concerns regarding the fairness of criteria such as age. Ultimately, policymakers must strive to develop and maintain frameworks and policies that can be consistently adapted to address the ongoing challenges and concerns raised by potential donors, patients and their families.
Sources
“Ethical principles in the allocation of human organs”. Organ Procurement & Transplantation Network. https://optn.transplant.hrsa.gov/professionals/by-topic/ethical-considerations/ethical-principles-in-the-allocation-of-human-organs/
“Philosophy of organ donation: Review of ethical facts”. National Library of Medicine. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4478599/
How Do OPTN and UNOS Work Together to Ensure Equity in the Transplant Process?
July 8th, 2025The United Network for Organ Sharing (UNOS) operates the Organ Procurement and Transplantation Network (OPTN), working collaboratively to ensure equity in the transplant process through multiple strategic efforts. Although UNOS and OPTN follow guidelines and policies that emphasize the prioritization of transparency and fairness in organ allocation, UNOS is also primarily responsible for developing policies and adopting policy changes to achieve more equitable outcomes. The OPTN can form committees or workgroups to research further measures to improve or enhance current outcomes, which can provide UNOS with the necessary data to make informed decisions for policy development.
UNOS and OPTN use the Equity in Access dashboard to track and maintain outcome data respective to demographics, allowing greater visibility and transparency regarding access to transplants. This data helps optimize organ allocation nationwide since one of the primary barriers to transplant access is the potential candidates’ location. The OPTN publishes this dashboard data in monitoring reports on organ allocation policies; likewise, the dashboard is instrumental in advancing public research. The UNOS acts as a facilitator in this regard, obtaining the necessary authorizations for the OPTN to collect the data included in the dashboard and other data vital to improving policy. UNOS uses the OPTN data to analyze trends and identify inequities in transplant patient populations.
UNOS and OPTN proactively engage with members and leaders in the transplant community to gather valuable insights and make collective decisions regarding organ allocation and transplant policies. This approach enables the UNOS and OPTN to consider various perspectives and concerns within the community, making it easier for stakeholders to develop equitable practices and guidelines. Through these collaborative efforts, UNOS and OPTN can prioritize essential factors such as compatibility, fairness and medical need to ensure that organs are allocated appropriately and have a high likelihood of transplant success.
Sources
“Access: Improve access to the transplant healthcare system”. United Network for Organ Sharing. https://unos.org/transplant/improve-organ-donation-and-transplant-system/transplant-access/
Does Health Insurance Pay for Transplant Surgery?
July 8th, 2025Typically, in the case of both living and deceased organ donation, the transplant recipient’s health insurance pays for transplant surgery and other medical services related to organ or tissue donation. However, many insurance plans have a maximum amount they will pay within a lifetime or for a specific procedure, known as a cap. Sometimes, secondary or supplementary insurance may cover the expenses that the recipient’s primary insurance does not cover. However, since the costs associated with transplant surgery can be substantial, lack of coverage may prevent potential recipients from receiving a transplant due to the inability to pay. In these cases, Medicaid may help cover the cost depending on where the recipient lives.
Following approval to receive transplant surgery, individuals with insurance coverage are encouraged to plan for the anticipated expenses by reviewing their health insurance policy to understand the costs covered. Contacting the insurance company is also highly encouraged to gain further insight into caps, co-pay, deductibles and reimbursement for additional services after the surgery. It can be helpful to ask the following questions about insurance coverage for transplants:
- Does my insurance plan have a maximum limit or cap for transplant service coverage?
- Is the transplant center or hospital in-network with this insurance plan?
- What deductibles apply to these transplant services?
- Is a prior authorization needed for coverage?
- Are there any requirements or restrictions regarding pre-existing conditions?
It is important to remember that any expenses not covered by the transplant recipient’s insurance must be paid for by the recipient using an alternative method. The donor and the donor’s family do not pay for any services associated with organ and tissue donation or transplant surgery. Financial coordinators and social workers at the hospital or transplant center can help provide potential recipients with access to resources and further information regarding options for payment.
Sources
“Living donor transplant”. Mayo Clinic. https://www.mayoclinic.org/tests-procedures/living-donor-transplant/living-donor-frequently-asked-costs-and-insurance-questions/gnc-20204089
“How to Get on the Waiting List for an Organ Transplant”. Verywell Health. https://www.verywellhealth.com/organ-transplant-waiting-list-requirements-3156951
“Transplant Services”. Florida Agency for Health Care Administration. https://ahca.myflorida.com/medicaid/medicaid-policy-quality-and-operations/medicaid-policy-and-quality/medicaid-policy/medical-and-behavioral-health-coverage-policy/primary-and-preventive-care-policy/transplant-services
“Resources for patients, caregivers, and the public”. UNOS. https://unos.org/resources/patient/
What Is the UNOS (United Network for Organ Sharing)?
July 8th, 2025The United Network for Organ Sharing (UNOS) is a private non-profit organization that manages the U.S. transplant system, otherwise known as the Organ Procurement and Transplantation Network (OPTN). UNOS was established in 1977 and is responsible for overseeing the coordination and distribution of donated organs through the OPTN. As a forum for donation and transplant professionals, UNOS fulfills three crucial roles:
- Improving the efficiency of the transplant system and processes
- Ensuring equitable access to suitable organs
- Increasing utilization of donated organs
Although UNOS manages the national transplant system and ensures effective matching of recipients to donors, it is not responsible for registering or removing patients on the waitlist for a transplant. UNOS operates a centralized computer network called UNet, which connects histocompatibility labs, transplant centers, and organ procurement organizations. This network provides a platform for patients to be listed and matched for transplants and housing the data required by the OPTN for compliance monitoring.
The UNOS coordinates the OPTN committees and the board of directors’ actions. It enables OPTN members to develop policies that inform the equitable distribution of organs and opens policy proposals for public comment. The UNOS also plays a significant role in educating transplant professionals and the general public. While the UNOS promotes awareness of the general public regarding the importance of organ donor registration and its life-saving capabilities, it also educates transplant professionals about their involvement in the overall donation and transplant process.
Since its formal incorporation in 1984, UNOS has taken substantial actions to ensure the transplant system is more robust and efficient. This has increased the number of suitable organs recovered from donors and the corresponding number of transplants performed. Its continuous partnership with leaders in science and technology has ensured that OPTN members and volunteers have access to the necessary resources and tools to achieve a timely donation and transplantation process. Through its work, UNOS maintains a pivotal role in saving and improving the lives of patients needing transplants nationwide.
Sources
“United Network for Organ Sharing FAQs”. United Network for Organ Sharing. https://unos.org/about/faqs/#WhatIsTheOPTN
“Organ Procurement and Transplantation Network Policies and Reports”. Health Resources & Services Administration. https://www.organdonor.gov/about-us/legislation-policy/optn
What Is the Organ Procurement & Transplantation Network (OPTN)?
July 8th, 2025The Organ Procurement and Transplantation Network (OPTN) is a nationwide transplant system. While it is not a government agency or entity, it operates under the oversight and contract of the federal government through the United States Department of Health and Human Services. The purpose of the OPTN is to carry out the functions outlined in the National Organ Transplant Act of 1984 and to improve the system further so that more individuals can access suitable organs for transplantation.
The OPTN is composed of professionals in the transplantation and donation system, as well as member organizations and individual members. Membership in the OPTN requires that organizations and institutions meet specific requirements set by the OPTN and that they actively contribute to the formation of policies that guide the transplant systems. These members contribute to decision-making in collaboration with committees and the OPTN board of directors. Members of the OPTN include, but are not limited to:
- Organ procurement organizations (OPO)
- Transplant hospital programs
- Transplant histocompatibility laboratories
- Voluntary health organizations
- Medical professional organizations
- Scientific organizations
- General public members (donor families, ethicists, etc.)
- Business members
Additionally, the OPTN manages organ allocation to patients based on factors such as urgency, proximity, compatibility and other relevant factors. As the infrastructure that connects members to facilitate fair access to organs, the OPTN also monitors the performance of OPOs and transplant centers to ensure that they remain compliant with federal regulations. Overall, the OPTN is vital in the support and advancement of organ transplantation throughout the United States.
Sources
“About OPTN”. Organ Procurement & Transplantation Network. https://optn.transplant.hrsa.gov/about/
“About OPTN membership”. Organ Procurement & Transplantation Network. https://optn.transplant.hrsa.gov/about/about-optn-membership/
How Long Does It Take to Process a Donation of Organs or Tissue?
July 8th, 2025The time necessary to process an organ or tissue donation varies, ranging from 24 to 36 hours to up to a few days. The tasks involved, such as evaluating donor suitability, gathering authorization, identifying potential matching recipients, and organ recovery and transplantation, can sometimes take several hours per task since there are so many logistical and medical factors to consider. It is crucial to place donations with the most compatible match possible to reduce the risk of rejection, which makes evaluation and identification tasks all the more time-consuming to achieve the ideal outcome.
Although the donation process can take a fair amount of time, organ transplants can only occur within a specific window of time to maintain the viability of the organ. Some organs are only viable for up to six hours after removal from the donor’s body. It can also take several hours to complete an organ transplant surgery.
In general, organ viability with preservation typically lasts:
- 2 to 4 hours for lungs
- 4 to 6 hours for hearts
- 12 to 18 hours for livers
- 12 to 18 hours for the pancreas
- 8 hours for intestines, and
- 48 hours for kidneys
With medical advancements, tissue donations tend to have much broader windows of viability, and many tissues can remain viable for years with proper preservation.
Ultimately, the donation process is driven by multiple factors and requires timely coordination among teams, patients and their families to be successful. After the donation process is complete, an ongoing follow-up process begins and typically continues for weeks or months, depending on the needs of the donor’s family.
Sources
“Deceased Donor Transplant Process.” New York-Presbyterian. https://www.nyp.org/transplant/organ-donation/organ-transplant-process
“Donation Process.” Donate Life Texas. https://www.donatelifetexas.org/donation-process/
“Organ Donation and Transplantation.” Cleveland Clinic. https://my.clevelandclinic.org/health/treatments/11750-organ-donation-and-transplantation
Is It Possible to Restrict Organ Donation From Prisoners or Other Groups?
August 6th, 2025Due to federal law, it is not possible to restrict organ or tissue donation from specific groups. Policies regarding donations from incarcerated individuals are frequently debated due to ethical concerns. Additionally, these policies are not standardized throughout the United States and vary across jurisdictions.
Only 40% of U.S. prison systems have accessible policies regarding donations. States like Alaska, Georgia, Idaho, and Arizona allow incarcerated individuals to make living donations to immediate family members. In contrast, Minnesota has a broader policy, which allows blood, marrow, or organ donation if it can potentially save someone’s life. Some states also specifically exclude donations from individuals with an execution warrant.
Some jurisdictions have designated policies for donations indicating that they can only donate while living, whereas others permit posthumous donation with prior registration or family consent. These policies are often informed by efforts to maintain autonomy among incarcerated individuals or to address any concerns regarding potential coercion. Ultimately, the landscape surrounding prison policies on organ donations is diverse and constantly evolving. As ethical debates around donations from incarcerated individuals continue, these policies are likely to remain in consistent development.
Sources
“Donation FAQs.” Donor Alliance: Organ & Tissue Donation. https://www.donoralliance.org/understanding-donation/donation-frequently-asked-questions/
“US prison policies on organ donation for individuals who are incarcerated.” JAMA Network Open. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9996393/
Can Someone Change Their Organ and Tissue Donation Status After Registration?
August 6th, 2025Yes, individuals can change their organ and tissue donation status after registration. Although the process for making changes varies depending on how the registration occurred, individuals can change their donor status at any time. If someone’s wishes regarding organ or tissue donation have changed, it is crucial to maintain updated documentation that reflects their current preferences. Anyone who registers to be an organ and tissue donor remains on their state’s registry unless they remove themselves by updating their status to indicate that they no longer wish to be a donor.
It is important to note that most Department of Motor Vehicles (DMV) do not allow donors to update or change their status. Individuals who are interested in changing their donor status should refer to their local state registry to provide updated information.
If registration occurred online, individuals can access their donor registry account and make the changes directly in their account. The online accounts for donor registration vary. Some states have their own sites, but there are also organizations, such as Donate Life America, that register donors in a national database. It is important to note that any updates made online will replace donor status records at the DMV, but will not result in reissued identification or licenses.
Changes in donor status should be communicated to family and loved ones and updated as needed in other appropriate documentation. For example, some states include preferences regarding organ and tissue donation in statutory advance directives, so it would be important to update any changes in donor status in those documents. Ultimately, whether deciding to update online or at the DMV, it is crucial to ensure that all documents that include donor status are consistent and aligned with personal preferences.
Sources
“Donation Facts.” Honor Bridge. https://honorbridge.org/about-donation/donation-facts/
“Organ Donation FAQ.” Health Resources & Services Administration. https://www.organdonor.gov/learn/faq
Does Race Matter in Organ Donations?
July 8th, 2025Organs are not matched according to race or ethnicity, and individuals from different races can match one another for organ donations. However, individuals who are waitlisted to receive a transplant are more likely to become recipients if there are more donors from the same racial or ethnic background. Tissue markers and blood type matches are more likely among individuals of the same ethnicity.
Organ transplants are more successful when made within the same ethnic group due to human leukocyte antigens. HLAs help regulate the immune system and are proteins in most body cells. When the HLA-type doesn’t match well, it can impact transplant outcomes and influence matching. For example, kidney transplants are most needed among African American patients. However, since HLA doesn’t match well between Caucasian and African American candidates and there are fewer African American donors, African American transplant candidates often need to wait longer to receive a suitable transplant match or receive a transplant that may not be an optimal match.
Diversity in the donor population helps to increase transplant access for everyone. It can also increase the likelihood of long-term survival when donors and recipients are closely matched. Ultimately, fostering diversity among the donor population, addressing cultural concerns, increasing awareness about the importance of donation, and promoting donation across all communities are essential components of a more equitable organ transplant system.
Sources
“Does race matter in organ transplants?” Donor Alliance: Organ & Tissue Donation. https://www.donoralliance.org/newsroom/donation-essentials/multicultural-groups-donation-does-race-matter-in-organ-transplants/
“Race, ethnicity, & donation.” Donate Life America. https://donatelife.net/donation/organ-donation-race-ethnicity/
“Your questions answered.” LifeSource: The Heart of Organ Donation. https://www.life-source.org/latest/does-my-race-ethnicity-matter-in-organ-donation/
How Are Transplant Recipients Matched With Donors?
July 8th, 2025The process of matching donors with transplant recipients is complex and contains many factors and “moving parts.” Considerations include:
- Which organs are available for transplantation
- Physical compatibility (blood type, height, weight and age)
- The location of the donor and recipient
- Medical urgency
According to the Department of Health and Human Services, the matching process begins when the regional organ procurement network is notified that a potential donor has died. While the medical team at the hospital continues efforts to preserve the organs through artificial means such as ventilator support, intravenous fluids and medicine to maintain blood pressure, the OPO enters the patient’s information into The Organ Procurement and Transplantation Network (OPTN) database, which operates on a set of nationally established rules. The computer system determines where and to whom each organ goes. Although the decision-making process is far from simple, the basic steps include the following:
- Eliminate all unsuitable candidates: The computer first eliminates any candidate who is an unsuitable recipient for any or all available organs due to blood type, age, height or weight.
- Prioritize by region: For the purposes of organ allocation, the U.S. is divided into 57 local Donation Service Areas and 11 regions. For all organs except hearts and lungs, organs are allocated first to the sickest patients in the region where the donor is located. If there is more than one potential recipient in equal medical need of a transplant in the region, the patient located in the same local Donation Service Area as the donor usually gets first dibs. If there is no potential recipient in the region, the search expands to the entire country.
- Hearts and lungs: Because hearts and lungs must be transplanted quickly after retrieval, they are allocated according to distance from the donor hospital versus by region.
- Consider size and age: Pediatric patients are generally prioritized over adults when an available organ is from a child. If there is no child on the waiting list, a pediatric organ may go to an adult.
- Other medical factors: In addition to blood type and medical urgency, the matching system uses a number of factors in determining the appropriate donor-recipient match. Many of these are specific to the organ involved.
- Kidney
- Time on waiting list
- Tissue compatibility (based on immune system markers)
- Pediatric status
- Prior living donation (patient had a kidney transplant from a living donor that failed)
- Distance from donor hospital
- Survival benefit
- Heart
- Medical urgency
- Distance from donor hospital
- Lung
- Survival benefit
- Medical urgency
- Time of the waiting list
- Distance from donor hospital
- Liver
- Medical need
- Distance from donor hospital
- Kidney
Organs are preserved to ensure their viability. However, the time between organ retrieval and transplantation is limited. In general, the maximum survival time for preserved organs is:
- Heart, lung — 4-6 hours
- Liver — 8-12 hours
- Pancreas — 12-18 hours
- Kidney — 24-36 hours
Sadly, an inordinate number of retrieved organs do not reach their destination in time due to what experts call an antiquated system that sends life-saving organs cross-country as cargo on commercial airlines. According to an NBC News report based on an investigation by Kaiser Health News and Reveal from the Center for Investigative Reporting, between 2014 and 2019, 170 organs were discarded because of flight delays.
Sources
“Lost luggage: How lifesaving organs for transplant go missing in transit”. NBS News. https://www.nbcnews.com/health/health-news/lost-luggage-how-lifesaving-organs-transplant-go-missing-transit-n1130891
“Organ Procurement and Transplantation Network Policies and Reports”. HRSA. https://www.organdonor.gov/about-us/legislation-policy/optn
“How organ allocation works”. OPTN. https://optn.transplant.hrsa.gov/patients/about-transplantation/how-organ-allocation-works/
What Is the Transplant Waiting List?
July 8th, 2025The national transplant waiting list is a database of all the people in the United States who are registered to receive an organ when one becomes available from a deceased donor. The United Network for Organ Sharing (UNOS) manages this list. Another name is added to the national transplant waiting list every 9 minutes. Currently, more than 100,000 people need a lifesaving organ transplant.
Once on this list, you may receive an organ quickly or wait many years to get one. Most transplant candidates wait for quite some time as there are not enough donor organs for everyone in need. Wait time is also affected by which life-saving organ is needed. Those waiting for a kidney generally wait an average of 3 to 5 years, while those waiting for a heart or lung might be matched in less than a year.
Organ allocation is not ranked by number, but rather computer-generated. Complex criteria are based upon location, medical urgency, survival benefit, and genetic compatibility of the recipient. Local patients receive preference, when possible, as the less time that elapses for organ transport, the greater chance of success. But those most in need are placed on an active waitlist and often given priority over others. Pediatric patients or prior living donors may be granted special consideration.
How do I get on the waiting list?
Once your healthcare specialist determines that you are, or may soon be, in organ failure, you will be referred to a transplant center in your area. Once there, a transplant physician will evaluate whether you qualify for organ transplantation.
There are several requirements you must meet to be placed on the national transplant waiting list. These may slightly differ depending on the organ you need, but generally, all cover some key elements. A medical team will first help to determine whether a living donor is an available option to you. You may still be placed on the waiting list even if there is a potential for one. A comprehensive physical examination, diagnostic testing, and lab studies will determine how well your organs are functioning and whether your decline warrants the need for transplantation. If not, you will be monitored and returned to the center for future testing when warranted.
If you are still considered a potential candidate, further testing will evaluate your ability to tolerate surgery. Any signs of other life-threatening conditions like heart disease, diabetes, infections, or cancer could disqualify you. Genetic testing will also be performed, so you can be matched with a donor organ. You will meet with financial counselors to ensure that you can afford the surgery, as well as the mandatory anti-rejection medications following transplant.
A full psychological evaluation will also be conducted to rule out any mental health issues that might interfere with your ability to adjust to life post-transplantation. Lastly, the medical team will monitor whether you are following a current medical regimen to maintain the best health possible while you wait for a donor organ. Any non-compliance, like drinking alcohol while treating liver disease or substance abuse disqualifies any potential candidate.
What happens after I get on the list?
Your transplant center will not notify you when you have been added to the national transplant waiting list. If you have any questions, you should reach out to your medical team at that center. You may have the ability to register with more than one center in your area to increase your chance of receiving an organ as a multiple listing. Be aware that you must be able to respond quickly and get to any center within hours if one becomes available to you. It is up to the patient to reach out to additional transplant centers in their area. They may or may not allow you to list with them as well.
Until it is your time to receive an organ, you are expected to follow physician’s orders and take good care of yourself. And even though it may not benefit you directly, perhaps encouraging everyone you know to become an organ donor could help someone else on the list.
Sources
“Frequently Asked Questions”. UNOS. https://unos.org/transplant/frequently-asked-questions/#Waiting
“Our Global Network of Partners”. National Marrow Donor Program. https://www.nmdp.org/what-we-do/partnerships/global-transplant-network
“Sign Up To Be An Organ Donor”. Health Resources & Services Administration. https://www.organdonor.gov/sign-up
What Are the Risks in Being a Living Organ Donor?
July 8th, 2025Being a living organ donor is a very noble thing to do. Although a person can live a long, healthy life with only one kidney, one lung or a portion of a liver, there are some risks involved. First, of course, are the “normal” risks of surgery and anesthesia. Removing an organ is a major procedure, and complications, such as bleeding, infection or delayed wound healing can occur. These are usually easily managed, however, and most donors are discharged from the hospital after a few days. According to data collected over the past 60 years, the risk of dying after donating a kidney is less than 0.03%, and the risk of major complications is less than 1%.
Additionally, there is the unlikely but real possibility that a kidney donor will suffer a catastrophic injury to their one remaining kidney. Or, more likely, that their remaining kidney will “give out” more quickly because it is doing the work of two. And, in fact, the incidence of kidney failure in people who have donated kidneys is higher than that of healthy individuals who have not. (It is still lower than the general population because kidney donors are carefully screened for chronic health conditions, while the general population includes many individuals who are chronically ill.) Still, the risk is quite small. According to one study from Norway, the incidence of end-stage renal disease in living kidney donors was less than 0.5% over 15 years.
Lastly, there are short-term financial issues that can impact living donors. In most cases, the cost of donation is covered by the recipient’s health insurance, but there are sometimes uncovered costs related to the surgery itself. Donors also must take time off from work (about a month on average after the surgery) and may be forced to use sick time or vacation time during that time. If they have to travel to the transplant center for evaluation and testing, those costs, including airfare, food and lodging, may be out of pocket as well. According to the Living Donor Toolkit from the American Society of Transplantation, the average living organ donor spends about $5,000 on out-of-pocket expenses. Financial help may be available, however, so check with the transplant center you are working with to learn if there are resources available to you.
Sources
“Reassessing Medical Risk in Living Kidney Donors”. https://www.kidneyregistry.com/wp-content/uploads/2021/03/Reassessing-Medical-Risk-in-Living-Kidney-Donors.pdf
American Society of Transplantation: Living Donor Toolkit: https://www.livingdonortoolkit.com
“Risk in Living Kidney Donors”. Journal of the American Society of Nephrology. https://pubmed.ncbi.nlm.nih.gov/30858158/
What Is Living Organ Donation?
July 8th, 2025As the term implies, living organ donation happens when a live person donates an organ to someone in need of a transplant. At the present time, the most common organ donated from one living person to another is a kidney. Nearly 6500 kidney transplants from live donors occurred in the U.S. in 2022 alone. A living person can also donate a portion of their liver. Since the liver is the only organ in the body that will regenerate, the donor’s liver grows to normal size again within a few months, while the transplanted liver tissue gives the recipient a new chance at life. More than 600 live transplants involving living donors occurred in 2022, setting an annual record. You may also be able to donate a lung or part of a lung, a portion of your intestines, or part of your pancreas. However, as of this writing, these transplants are quite rare.
According to the United Network for Organ Sharing, there are two paths to live-donor organ donation: Directed donation and paired donation. In directed donation, the donor specifies who is to receive the donated organ. This most often occurs when the donors are related by blood, (for example, siblings or a parent and child) since they are more likely to be an immunological match. However, it’s possible for an unrelated donor, such as a spouse or friend, to donate an organ if their blood and tissue types match the recipient. According to the University of Utah Transplant Center, one in four donations from living donors are from people who are not biologically related to the recipient.
Paired donation, on the other hand, is a pilot project sponsored by the Organ Procurement and Transplant Network that matches people who are willing to donate a kidney with unrelated recipients who need them. In far too many cases, a healthy person wants to donate to a friend or relative who is on the transplant waiting list, but is not a tissue or blood type match. The pilot program collects data on these individuals and matches potential donors with potential recipients by blood and tissue type. (See diagram below) At this time, kidneys are the only organs that are matched this way.
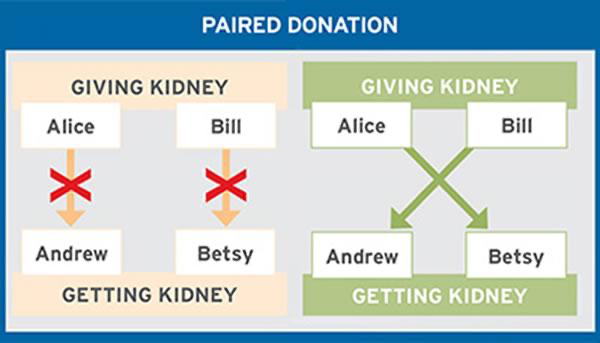
In the above example, Bill wanted to donate to Betsy and Alice wanted to donate to Andrew, but neither was a match. All four people were entered into the registry, and the computer matched Bill and Andrew and Alice and Betsy by tissue and blood type.
Sources
“Living Donation”. United Network for Organ Sharing. https://unos.org/transplant/living-donation/
“Kidney Paired Donation”. Organ Procurement & Transplantation Network. https://optn.transplant.hrsa.gov/professionals/by-organ/kidney-pancreas/kidney-paired-donation/
Who Pays for Organ Donation Surgery After Death?
July 8th, 2025The surgery used to recover a donated organ after the donor dies is typically covered by the organ procurement organization or OPO. This organization assumes responsibility for the costs to recover and process donated organs and tissues after the donor’s death. If an OPO does not cover this cost, the recipient of the donated organs or tissues may pay for the surgery. The donor’s family or estate is not charged for any medical expenses associated with donation, but is responsible for the cost of end-of-life care prior to the donor’s death and final arrangements for funerals, burials or cremations after death.
When an OPO is responsible for the cost of procurement, it is later reimbursed by the transplant center or hospital that will receive the organ for the upcoming procedure. If tissues are donated instead of organs, the OPO is reimbursed by the tissue processor instead. The transplant center or hospital will then bill the recipient for the cost of the procedure after the transplant has occurred, which is usually either covered by the recipient’s insurance or alternative financial arrangements that the recipient has made. Organ donation recipients often have to provide financial proof establishing that they are able to uphold their portion of the financial responsibility for any medical expenses associated with the donation and subsequent transplant.
Sources
“Get the Facts: Are My Family or My Estate Ever Charged for Donation?”. Donor Alliance. https://www.donoralliance.org/newsroom/donation-essentials/get-facts-family-estate-ever-charged-donation/
“Organ donation: Don’t let these myths confuse you”. Mayo Clinic. https://www.mayoclinic.org/healthy-lifestyle/consumer-health/in-depth/organ-donation/art-20047529
How Does Organ Donation After Death Work?
July 8th, 2025When a loved one’s organs are donated after death, a series of steps is taken to ensure that the organs are suitable and will remain viable for successful transplantation. In accordance with federal regulations, the hospital will reach out to a local Organ Procurement Organization (OPO) to notify them that your loved one is near death or has died. A physician will be present to conduct a brief test to confirm brain death and will also note the time of death per the requirements for organ donation.
Before the OPO can move forward with organ donation, consent must be acquired. If your loved one’s name is listed in the state’s organ donor registry, it is considered legal consent. Other methods to determine consent include reviewing your loved one’s driver’s license or other documentation. Sometimes the OPO may need to contact the next of kin as well. After approval is granted, the OPO will gather your loved one’s medical and social history for a medical evaluation. This evaluation determines whether your loved one’s organs can be donated.
The OPO official and a medical team will review the overall condition of your loved one’s organs and a transplant surgical team will begin removal if the organs are in suitable condition. The surgical team is responsible for removing organs and approved tissues. Any incisions or cuts that are made during the procedure will be closed to ensure that an open-casket funeral can be held if it is the patient’s or family’s preference. The OPO often works with the funeral director at the funeral home to ensure that these wishes are honored.
Assuming the evaluation reflects that the organs are suitable for donation, the OPO will contact the Organ Procurement and Transplantation Network (OPTN), which is the national transplant database that houses information about patients on the waitlist in need of a transplant. The OPO will input your loved one’s information into the system to identify patients that match your loved one’s donation per organ. Each organ is offered to the transplant team of the patient that is deemed to be the most suitable match and then the transplant surgeon from that team determines whether it is appropriate to proceed with the transplant.
In the weeks that follow, the OPO conducts follow-up outreach to the donor’s family to let them know which organs were transplanted. The names of the recipients are kept private, although there are communication guidelines in place if the donor’s family and the recipients wish to interact with each other. As time progresses, the OPO may provide additional support to the donor family, such as resources for bereavement counseling or assistance with memorial events.
Sources
“Deceased Donation”. United Network for Organ Sharing. https://unos.org/transplant/deceased-donation/
“Donation After Life”. Health Resources & Services Administration. https://www.organdonor.gov/learn/process/donation-after-life
What Is Donation After Cardiac Death (DCD)?
July 8th, 2025Donation after cardiac death (sometimes called donation after circulatory death) or DCD is organ donation that occurs when a person is in an irreversible coma but doesn’t meet the strict criteria for brain death. When organ transplantation first became a reality in the 1950s and 1960s, all organ transplants were donations after cardiac death because the criteria for brain death [link to What is brain death?] were not developed until 1968. First presented in a landmark paper “A definition of irreversible coma, the Report of the Ad Hoc Committee of the Harvard Medical School to Examine the Definition of Brain Death,” those criteria are credited with laying the groundwork for deceased donor organ transplantation as it exists today.
Prior to donation after cardiac death, the next of kin or healthcare agent is first consulted to discuss the possibility of removing a person who doctors have determined has no hope of survival from ventilator support. This discussion should happen independently of any discussion about organ donation unless the family mentions the option to the physician first. If the family agrees, the hospital contacts the Organ Procurement Organization, which will work to find a suitable recipient or recipients. Once suitable candidates are located, the person is taken to the operating room, and preparations to remove the organs are made.
Once the OR team is ready, the patient is taken off ventilator support and observed. When the heart stops beating (which usually happens fairly quickly), doctors wait an additional 5 minutes to ensure that a spontaneous heartbeat doesn’t return. At that time, a team of specialists removes the abdominal organs, such as the liver, kidneys, pancreas, and intestines.
Advances in technology and evolving organ donation guidelines have made it possible for the heart and lungs to be transplanted following cardiac death. Because organ viability depends on the circumstances of death, rigorous evaluations and strict criteria must be met before transplantation can proceed. Despite these challenges, donation after cardiac death (DCD) is growing more frequent, providing a vital lifeline for patients awaiting transplants.
Sources
“‘Donation after cardiac death’: New heart transplant method being tested for the first time in the U.S.”. Stat News. https://www.statnews.com/2020/01/16/heart-transplant-donation-after-cardiac-death/
“How Donation after Cardiac Death is Changing the Transplant Landscape”. Emory Healthcare. https://www.emoryhealthcare.org/stories/heart-health/donation-after-cardiac-death-is-changing-the-transplant-landscape
“Critical Pathway for Donation After Cardiac Death”. United Network for Organ Sharing. https://unos.org/wp-content/uploads/Critical_Pathway_DCD_Donor.pdf
What Is Brain Death?
July 8th, 2025The term “brain death” confuses many people because it implies that a person who has died is actually alive. However, a person who is brain dead has no brain function, and without brain function, the rest of the body cannot survive. They cannot breathe or maintain a heartbeat without the aid of a ventilator.
Brain death typically occurs after a severe head injury, bleeding in the brain, or an event that deprives the brain of oxygen, such as drowning or prolonged cardiac arrest. It can occur almost immediately, or it can happen over a period of hours or days as injured brain tissue swells.
In accordance with the Uniform Determination of Death Act, doctors determine brain death through a series of physical examinations and diagnostic tests. They check for spontaneous breathing, response to painful stimuli, and whether or not the pupils respond to light. They also perform an electroencephalogram, or EEG, and another test that shows if there is any blood circulating in the brain. If the EEG shows no activity, there is no blood flow to the brain, and the person can no longer breathe or move on their own, the person is declared dead. In most states, two doctors must certify the death.
After death has been determined, a potential organ donor will be kept in the ICU on a ventilator and receive specialized care to ensure organ function is maintained. At the same time, the Organ Procurement Organization in the region is notified and supplied with relevant details about the patient, such as age, sex, blood type, height and weight. When the OPO identifies a suitable recipient(s)[link to How are donors and recipients matched?] the patient is taken to the operating room and the organs to be donated are removed by a specially trained surgical team.
Sources
“What is the Uniform Determination of Death Act (UDDA)?” FindLaw. https://www.findlaw.com/healthcare/patient-rights/what-is-the-uniform-declaration-of-death-act-or-udda.html
“The diagnosis of brain death”. Indian Journal of Critical Care Medicine. https://pmc.ncbi.nlm.nih.gov/articles/PMC2772257/
Can Someone Donate Organs and Tissues If They Have Selected Medical Aid in Dying?
July 8th, 2025It is not yet possible for individuals to donate their organs and tissues following medical aid in dying, although this may change in the future. While the practice of organ and tissue donation after medical aid in dying (MAID) is becoming increasingly common in Belgium, the Netherlands, Canada and Spain, this combined procedure remains a new concept in the United States. The decision to donate organs and tissues after selecting MAID introduces ethical considerations surrounding patient autonomy, non-maleficence and vulnerability. These concerns can be challenging to navigate in a country where the practice of MAID is less widespread compared to other countries where it is more socially and legally accepted.
It is important to note that organs and tissues generally remain viable after medical aid in dying, and the decision to die by this practice typically would not damage organs and tissues that might otherwise be suitable for transplantation. Cases in the Netherlands have demonstrated success in procuring organs such as livers, kidneys and lungs. Difficulties in effective implementation generally pertain to logistics and additional time investment from medical staff. Similar to any other organ or tissue donation process, it is crucial for the organs to be procured as soon as possible after the donor has died.
As perspectives and policies about medical aid in dying continue to evolve, the ethical considerations associated with it in relation to organ and tissue donation will also likely change.
Advocates for MAID will likely need to look to its efficacy and implementation in other countries as evidence-based examples of what donation practices and policies may involve in the future. Ultimately, patients’ end-of-life decisions and autonomy must be respected and upheld with utmost importance.
Sources
“Directed Organ Donation After Euthanasia”. Frontiers. https://www.frontierspartnerships.org/journals/transplant-international/articles/10.3389/ti.2023.11259/full
“Organ Donation after Medical Assistance in Dying — Canada’s First Cases”. New England Journal of Medicine. https://www.nejm.org/doi/full/10.1056/NEJMc1915485
“Organ donation after medical assistance in dying at home”. Canadian Medical Association Journal. https://pmc.ncbi.nlm.nih.gov/articles/PMC6217602/
If a Family Member Needs an Organ at the Time of My Death, Can I Donate to Them Specifically?
July 8th, 2025Yes, a donor may donate their organ to a specific individual, such as a family member. This is typically known as a directed donation or designated donation. Directed donations may include organs and tissues donated by living donors or those who have died. If the person who died was a donor and did not indicate a preference regarding who receives their organs, the donor’s family may manage the directed donation instead.
It is important to note that requesting to donate to a specific person does not guarantee that a transplant will occur, since additional testing must be conducted to determine if the recipient is a match for the loved one’s organ. If the individual is not a match for the designated organ, the organ will be donated to another recipient on the National Transplant Waitlist. Directed donations are the most common type of living donation. Donors who provide living donations can be:
- A biological relative (parent, sibling, or adult child)
- A biologically unrelated person (friend, coworker, or partner)
- A biologically unrelated person aware of a candidate’s need
Overall, the intention to improve a family member’s health outcome by providing an organ donation is an honorable gesture. Since it cannot be guaranteed that these organs will be an appropriate match for the intended recipient, individuals considering directed donations are encouraged to be open to the possibility of their donations being distributed to those in greatest need. Potential donors are advised to contact a local organ procurement organization or transplant center for more information about the most appropriate options based on their respective circumstances.
Sources
“Frequently asked questions about organ donation.” Gift of Life Donor Program. Accessed 18 September 2024. https://www.donors1.org/learn-about-organ-donation/how-does-organ-and-tissue-donation-work/frequently-asked-questions/
“Living donation.” UNOS. Accessed 18 September 2024. https://unos.org/transplant/living-donation/
“What is directed donation?” LifeSource. Accessed 18 September 2024. https://www.life-source.org/latest/what-is-directed-donation/
Can Certain Medical Conditions Prevent Someone From Becoming an Organ or Tissue Donor?
July 8th, 2025Some medical conditions, such as active infections and certain chronic diseases, can prevent a person from becoming an organ or tissue donor. However, nothing prevents someone from registering as a donor, regardless of their health status. Individuals are encouraged to register even if they have chronic conditions. This is because doctors who handle organ donation do not determine whether someone is medically suitable to donate until the time of death.
Suitability for donation is determined on a case-by-case basis since circumstances can vary among patients. However, some examples of conditions that often preclude donation include the following:
- HIV or AIDS
- Hepatitis
- Pneumonia, sepsis or other infections at the time of death
- Lymphomas
- Cancer
- Autoimmune diseases
- Cruetzfeldt-Jakob disease
- West Nile virus
- Chagas
- Malaria
- Herpes (active)
- Rabies
Additionally, although some health conditions may affect the viability of specific organs, all organs and tissues are rarely unusable. For example, even if someone has a chronic disease that prevents the donation of an organ like a heart or kidneys, other organs or tissues can likely be used. Doctors will conduct tests and evaluate the viability of each of a potential donor’s organs and tissues to determine if there are any that may still be appropriate for donation if there has been substantial damage from a chronic disease. If, for example, a person had metastatic cancer within the previous five years, they may not be appropriate for donating organs or most tissues, but they could still donate their corneas.
Sources
“Organ donation: Don’t let these myths confuse you”. Mayo Clinic. https://www.mayoclinic.org/healthy-lifestyle/consumer-health/in-depth/organ-donation/art-20047529
“What Factors Disqualify People From Being Organ Donors?” Forbes. https://www.forbes.com/sites/quora/2018/12/14/what-factors-disqualify-people-from-being-organ-donors/?sh=740bf2a0759e
“Would Certain Conditions or Diseases Make You Ineligible to Donate?” Life Source. https://www.life-source.org/latest/would-certain-conditions-or-diseases-make-you-ineligible-to-donate/
Is Organ/Tissue Donation Possible When Someone Dies at Home?
July 8th, 2025Organ donation usually isn’t feasible when someone dies at home, due to the logistics of transportation and coordination, and the short time most organs are viable after death. Vital organs such as the heart or liver only remain viable and appropriate for transplantation for a certain number of hours after a potential donor has died. Some examples of how long vital organs can remain viable include:
- Heart: 4 to 6 hours
- Lungs: 2 to 4 hours
- Liver: 12 to 18 hours
- Pancreas: 12 to 18 hours
- Kidneys: up to 48 hours
Due to these extremely limited time frames, only people who are in the hospital on ventilator support are usually candidates for donating vital organs.
Although organ donation isn’t possible, tissue donation may be an option when someone dies at home because tissues have a different timeline for viability. Tissues such as corneas, heart valves, veins, tendons and many others can typically be removed from the donor up to 24 hours after the person dies. Additionally, once removed from the donor, tissues have greater longevity than organs since they can be processed and stored for extended periods prior to transplantation.
Ultimately, if donation is an interest and the potential donor has a preference of dying at home, it’s essential to develop a plan of how to properly handle the process ahead of time. This may include contacting a local tissue bank or organ procurement organization to ensure that they are equipped and qualified to handle the donation process.
Organizations such as the National Donate Life Registry can also provide additional information on how to plan ahead for tissue or organ donations. By proactively researching these options, individuals may be able to ensure that their wishes are communicated and honored.
Sources
“Frequently Asked Questions About Organ Donation for Older Adults”. National Institute on Aging. https://www.nia.nih.gov/health/organ-donation/frequently-asked-questions-about-organ-donation-older-adults
“What is the Time Frame for Transplanting Organs?”. Donor Alliance. https://www.donoralliance.org/newsroom/donation-essentials/what-is-the-time-frame-for-transplanting-organs
“Tissue Donation”. Donate Life. https://donatelife.net/donation/organs/tissue-donation/
“National Donate Life Registry”. Donate Life. https://donatelife.net/donation/donor-registries/national-donate-life-registry/
Who Can Donate Organs or Tissue?
July 8th, 2025As a rule, anyone who is over 18 can register to be an organ donor, and parents and guardians can authorize donation from children under 18. According to the Mayo Clinic, there are very few medical conditions that automatically disqualify a person from donating organs or tissue, and no one is automatically disqualified based on age. Additionally, since the passage of the HIV Organ Policy Equity (HOPE) Act in 2013, the organs from HIV-positive donors can now be transplanted into recipients with HIV.
Living organ donors are generally screened for underlying medical conditions before they can donate because they will need to be healthy enough to tolerate the surgery and recovery period. Although very few conditions will automatically exclude you, a history of uncontrolled hypertension, diabetes, or certain infections could prevent you from donating until they are under control.
Nor is age necessarily a factor in whether or not you can donate. The suitability of an elderly person’s organs might be evaluated more carefully than that of a younger donor, but transplants from people in their 60s and 70s have occurred. Even if you’re not suitable as an organ donor, your tissues may be used no matter what your age. Doctors will always try to use whatever organs and tissues they can to help save and improve lives.
With that being said, it’s important to know that deceased organ donation is only possible when a person dies under certain limited circumstances. Because organs begin to die almost immediately after heart function stops, they will not remain viable unless breathing and circulation are continuously maintained through artificial means. To accomplish this, a person who has suffered a cardiac arrest must receive CPR within minutes of death and be admitted to a hospital and placed on a ventilator soon after that. They must then be maintained on ventilator support until the organs can be recovered, after brain death or cardiac death is declared.
Sources
“HIV Organ Policy Equity (HOPE) Act is Now Law”. The White House. https://obamawhitehouse.archives.gov/blog/2013/11/21/hiv-organ-policy-equity-hope-act-now-law
How Common Is Organ Donation?
July 8th, 2025Thanks to greater public awareness and an increasing number of people willing to donate their organs, the number of organ transplants in the U.S. has been increasing each year. In 2024, U.S hospitals performed a new annual record of over 48,000 transplants from over 24,000 donors, averaging 132 transplants per day. These donations came from 16,988 deceased donors and 7,030 living donors.
The most commonly transplanted organs are kidneys, followed by:
- Liver
- Heart
- Lung
- Pancreas
- Kidney/pancreas
- Intestine
- Heart/lung
- Vascularized allograft transplants (VCA) – such as transplants of hands or faces
Yet, even given these promising numbers, the demand for organs far exceeds the supply. As of May 2025, there are nearly 104,000 people awaiting life-saving organ transplants in the U.S. At any given time, around 90,000 people are waiting for a kidney transplant, which can take an average of three to five years to receive. Sadly, many of those people–about 17 per day–will die before an organ becomes available. Meanwhile, a new name is added to the organ transplant waiting list every eight minutes. Still, progress has been continuing in the drive to find new organs. As of 2025, 60% of American adults are registered organ donors. This is due in large part to online registration systems and the ability to sign up as an organ donor at the DMV.
Sources
“Organ donation from deceased donors continues 12-year record-setting trend”. United Network for Organ Sharing. https://unos.org/news/2022-organ-transplants-again-set-annual-records/
“’Opt Out’ Policies Increase Organ Donation”. Stanford. https://sparq.stanford.edu/solutions/opt-out-policies-increase-organ-donation
“How many people are organ donors?” Donor Alliance. https://www.donoralliance.org/newsroom/donation-essentials/how-many-people-are-organ-donors/
“90,000 people are waiting for a kidney. Here’s one way to get them a kidney faster.” United Network for Organ Sharing. https://unos.org/news/90000-people-are-waiting-for-a-kidney-heres-one-way-to-get-them-a-kidney-faster/
“Organ Donation Facts and Statistics”. Donort Network West. https://www.donornetworkwest.org/about-donation/organ-donation-facts-statistic
Is There an Age Limit to Become an Organ Donor?
July 8th, 2025There is no age limit for organ and tissue donation. Anyone who is at least 13 years of age can register online, although the final decision is that of the legal guardian(s) until age 18. Additionally, anyone of any age can select “YES” when applying for or renewing their driver’s license or ID at the DMV. Since age is not a factor, people should not rule themselves out as potential donors – there has been a 93-year-old kidney donor and a 99-year-old cornea donor!
Though there is no set maximum age for being a donor, medical professionals will assess each organ individually at the time of death to determine if it is suitable for donation. Even if you are in your 70s, 80s or even 90s, you can still potentially donate your organs if they are in good working order. If an organ has been damaged by disease or aging, it might not be suitable for transplantation.
Further, donated organs and tissue from those aged 50 to over 80 are often in high demand by medical researchers. These may be donated through an organ procurement organization, which will arrange to have usable tissue removed within 24 hours of death. Whole body donation through a non-anatomical donation organization is another way to ensure that your or a loved one’s organs and/or tissues reach medical researchers.
Sources
“Organ Donation FAQ”. Health Resources & Services Administration. https://www.organdonor.gov/learn/faq
“Consumer Health”. Mayo Clinic. https://www.mayoclinic.org/healthy-lifestyle/consumer-health/in-depth/organ-donation/art-20047529
“A 95-year-old man just became the oldest organ donor in US history”. CNN. https://www.cnn.com/2021/05/12/health/oldest-organ-donor-wellness-trnd/index.html
“Organ Donation”. New York-Presbyterian. https://www.nyp.org/transplant/organ-donation/organ-donation-facts
“5 Things to Know About Organ Donation After Age 50”. AARP. https://www.aarp.org/health/healthy-living/organ-donation-age-limit/
“Non-transplant Anatomical Donation”. AATB. https://www.aatb.org/nados
Why Should I Register as an Organ and Tissue Donor?
July 8th, 2025The decision to register as an organ and tissue donor can extend and save lives, as well as improve the quality of life for other individuals. Donation is often the deciding factor between life and death for individuals who need a transplant. Someone is added to the organ wait list every 10 minutes, and 17 people die every day while waiting for a suitable match for an organ transplant.
Becoming an organ and tissue donor allows you to make a positive impact on someone’s life even after your death. Each donor has the potential to save eight lives and improve the quality of life for over 75 additional individuals. Your donation has the potential to allow transplant recipients to regain their health and mobility, increase their independence, reduce or alleviate pain or improve their overall well-being.
Registering as an organ and tissue donor may also provide comfort and a sense of peace to bereaved family members after your death. The realization that your organs and tissues are going to help other people can demonstrate that there is a silver lining despite the difficulty of experiencing the loss. It can also be a powerful reminder of a legacy of compassion for others — a legacy that can extend into the lives that have been saved and improved through that initial choice to become an organ and tissue donor.
There is a constant and ongoing demand for organ donors due to the significant number of organs needed in contrast to the immense shortage of suitable organs. Your decision to donate may mean offering a chance at a better life to someone who has waited for an organ donation for years. Ultimately, your decision to become a donor can be a final act of generosity with boundless opportunities to save and change lives.
Sources
“Organ Donation Facts and Statistics”. UC Health. https://www.uchealth.com/en/media-room/articles/organ-donation-facts-and-statistics
“Organ Donation Statistics”. Health Resources & Services Administration. https://www.organdonor.gov/learn/organ-donation-statistics
Should I Tell My Loved Ones About My Decision to Donate Organs or Tissues?
July 8th, 2025Although sharing your decision to become an organ or tissue donor is a personal choice, experts recommend that you discuss it with your loved ones. Choosing to have an open conversation about your decision can ensure that your wishes will be respected and upheld after your death. It also provides your loved ones with the opportunity to understand the rationale behind your decision, which they might otherwise struggle to understand without having the additional context from your discussion.
Since some individuals may have concerns surrounding organ and tissue donation, talking about it ahead of time can help alleviate confusion and provide them with peace of mind regarding your choice. People are often hesitant about the topic of organ and tissue donation due to the myths about the donation process. Discussing your decision with your loved ones creates the opportunity for dialogue regarding common questions or concerns that they may have, such as implications for medical care or final arrangements.
Finally, sharing your decision to donate your organs or tissues allows you to discuss the impact that your decision to donate has on other people’s lives. When an organ donor dies, they can save up to eight lives with their donated organs and more than 75 lives with donated tissues. Lives can be saved by being a match to patients who are on a transplant wait list, transitioning patients from dialysis, or providing skin and other important tissues that are essential in recovery from burns, blindness, trauma, reconstruction, and more.
Sources
“Frequently Asked Questions About Organ Donation for Older Adults”. National Institute on Aging. https://www.nia.nih.gov/health/organ-donation/frequently-asked-questions-about-organ-donation-older-adults
“Organ donation: Don’t let these myths confuse you”. Mayo Clinic. https://www.mayoclinic.org/healthy-lifestyle/consumer-health/in-depth/organ-donation/art-20047529
“6 Quick Facts About Organ Donation”. Penn Medicine. https://www.pennmedicine.org/news/six-quick-facts-about-organ-donation?path=News&path=six-quick-facts-about-organ-donation
Can My Family Override My Request to Be an Organ Donor?
July 8th, 2025Generally, families cannot override consent for organ donation. If an individual specified their desire to donate organs or tissue in an advance directive for healthcare or a legally executed will or was registered as a donor with the state, they are said to have granted “first-person consent” for donation after death. In every state in the U.S, the next of kin and/or authorized healthcare agent are barred from revoking first-person consent unless they have proof that the person revoked consent themselves. The only exception to this rule is if the potential donor was an unemancipated minor (for example, a 16-year-old child who signed up on the donor registry upon obtaining a driver’s license.) In that case, one or both parents may revoke consent.
With that being said, if you want to be an organ and/or tissue donor, tell your family, your healthcare agent and your friends. This is the best way to avoid conflict and confusion at an already difficult time. It will also allow you to explain why donating is important to you and discuss any questions your family may have. The process goes much more smoothly and will be less traumatic for everyone involved if your family knows your wishes in advance.
Sources
“First Person Consent”. United Network for Organ Sharing. https://unos.org/wp-content/uploads/unos/registires_combined.pdf
“Frequently Asked Questions About Organ Donation for Older Adults”. National Institute on Aging. https://www.nia.nih.gov/health/organ-donation/frequently-asked-questions-about-organ-donation-older-adults#
Who Can Consent to Organ or Tissue Donation If I’m Not a Registered Donor?
July 8th, 2025Although state laws may vary somewhat, under the Revised Uniform Anatomical Gift Act a designated healthcare agent or next of kin can consent to organ donation for a person who did not consent before their death. The act defines the decision-making hierarchy as follows:
- Healthcare agent or Power of Attorney
- Spouse
- Adult children
- Parents
- Adult Siblings
- Adult grandchildren
- Grandparents
- Adults who exhibited special care or concern, except those who provided compensated health care for that individual (for example, a doctor)
- Legal guardian
- Whoever has the legal authority to dispose of the body
In some states, however, one individual may not make the determination if another person in the same class objects (for example, two adult children disagree). If that is the case, the majority of individuals in that class or subsequent classes must agree before the donation can proceed. So, for example, if three adult children survive the deceased and there is no surviving spouse, two of the surviving children must agree to donate the person’s organs over the objections of the third before the process can proceed. If there are only two adult children and they disagree, a parent of the deceased person can “break the tie.”
Additionally, according to the National Academies of Sciences Engineering Medicine, many states allow a medical examiner or coroner to remove corneas from bodies that have come under their authority (for example, to perform an autopsy to determine the cause of death). These laws do not require express consent of the family or the person who has died.
Can Family Override Consent?
If an individual specified their desire to donate organs or tissue in an advance directive for healthcare or a legally executed will or was registered as a donor with the state, they are said to have granted “first-person consent” for donation after death. In every state in the U.S, the next of kin and/or authorized healthcare agent are barred from revoking first-person consent unless they have proof that the person revoked consent themselves. The only exception to this rule is if the potential donor was an unemancipated minor (for example, a 16-year-old child who signed up on the donor registry when acquiring a driver’s license). In that case, one or both parents may revoke consent.
With that being said, if you want to be an organ and/or tissue donor, tell your family, your healthcare agent, and your friends. This is the best way to avoid conflict and confusion at an already difficult time. It will also give you an opportunity to explain why donating is important to you and discuss any questions your family may have. The process goes much more smoothly and will be less traumatic for everyone involved if your family knows your wishes in advance.
Sources
“Presumed Consent”. National Academies: Sciences, Engineering, Medicine. https://nap.nationalacademies.org/read/11643/chapter/9#228
“First Person Consent”. United Network for Organ Sharing. https://unos.org/wp-content/uploads/unos/registires_combined.pdf
How Do I Register as an Organ or Tissue Donor?
July 8th, 2025At this time in the U.S., there are four ways to register to be an organ or tissue donor.
- Register when you apply for or renew a driver’s license. According to the Department of Health and Human Services, every state and the District of Columbia allows you to register as an organ donor when you apply for or renew your driver’s license. Most states give you the option to indicate which organs or tissues you want to donate.
- Register on your state donor registry. Every state in the U.S. maintains a central database of registered organ donors. To sign up in your state, click your state on Organdonor.gov and you will be taken to the registration form for your state. If you signed up when you got your driver’s license, you DO NOT need to register again. However, you can view your profile and make changes to your registration on the state donor registry at any time. However, if there is a “donor” designation on your driver’s license and you revoke consent in the registry, you may need to request a new driver’s license that indicates your new status.
- Register online at Donate Life America, the organ donation national registry. This information will be shared with the registry in your state.
- Sign up using the iPhone Health app: Using the Medical ID feature, you can sign up with Donate Life America by clicking an option and filling out a form. Your registration will go to your state donor registry and appear on your phone, where you, medical staff and first responders can access it.
In addition to signing up in your state’s registry, it’s also important to tell your loved ones and healthcare agent that you want to donate so they can honor your wishes when you die. According to Donate Life California, 72% of Americans who are eligible to donate organs at the time of their death do so, even if they did not register as an organ donor before. This is almost entirely because families feel certain that their loved one would want to donate their organs to save other lives.
Sources
“Sign Up To Be An Organ Donor”. Health Resources & Services Administration. https://www.organdonor.gov/sign-up
“National Donate Life Registry”. Donate Life. https://registerme.org/
What Is the History of Organ and Tissue Donation?
July 8th, 2025The history of organ and tissue donation in the United States dates back to the 1950s. After years of failed attempts, the first successful human organ transplant occurred in Boston, Massachusetts when 23-year old Ronald Herrick donated a kidney to his identical twin brother, Richard, on December 23, 1954. The procedure opened a new avenue of hope for thousands of Americans with otherwise untreatable life-threatening conditions. Sixty-eight years following that famous day, the United States surpassed its one millionth organ transplant in September 2022. This success was made possible by advancements in science, technology and policies that continue to pave the way for improvements.
Early 20th Century Milestones
Although a few experimental tissue transplants in animals occurred in the United States prior to the 20th century, most were unsuccessful. In 1912, surgeon Alexis Carrel was awarded the Nobel Prize for his pioneer work on blood vessel suturing and organ transplantation in animals. This was reportedly the first successful homograft, or same species transplantation. Although the credibility of his experiments is questioned by some, Carrel is considered a trailblazer in organ transplantation.
The early 20th century brought further experimentation around the world, including failed dog kidney transplantation. It was not until the early 1950s that homograft transplantation was even mildly successful in humans.
The more modern era of organ and tissue transplantation stems from a zoologist named Peter Medawar. In Medawar’s effort to understand why transplants between species were always rejected, he discovered that grafts exchanged between bovine fraternal twins were routinely accepted. Due to this discovery, Medawar was able to identify the immunological reaction that is the basis of rejection. In the early 1950s, this allowed surgeons to perform that landmark kidney transplant surgery between identical twins Ronald and Richard Herrick in 1954.
Key organ transplantation protocols and procedures established in the 1960s
Although most patients survived less than one year due to rejection of the kidney in the early 1960s, small advancements in immunosuppression were made and survival rates slowly increased.
Clinical advancements in transplantation that occurred in this decade include the following:
1962 – First successful kidney transplant from a deceased organ donor
1963 – First organ recovered from a brain-dead donor
1963 – First successful long-term immunosuppression achieved
1966 – First successful pancreas transplant performed
1967 – First crossmatch text for kidney transplant donors and recipients introduced
1967 – First successful liver transplant performed
1967 – First successful heart transplant from a donor after cardiac death (DCD) performed
Three key government milestones followed suit in 1968
- The Uniform Anatomical Gift Act was approved, which established the right of a decedent or family member to donate organs after death and codified the first legally recognized Uniform Donor card
- The first organ procurement organization, New England Organ Bank, was established to identify deceased donors in a local area
- The first definition of “brain death” based on clinical criteria became law in all 50 states.
Transplantation advancements in the final decades of the 20th century
The 1970s did not produce much in the way of further advancement. In the 1980s, organ preservation and cold storage were improved and new immunosuppressive drugs were introduced to reduce incidents of organ rejection. In the early 80s, the first single-lung transplant, as well as several double-transplant organs or tissues were successfully performed.
The National Organ Transplant Act was passed in 1984, federally regulating the medical field of organ donation and transplantation. This policy was responsible for the creation of the Organ Procurement and Transplantation Network (OPTN) to ensure a fair and safe system for allocation, distribution, and transplantation of donated organs. OPTN is a unique public-private partnership that continues to function as the main hub for all transplantation professionals and organizations in the U.S. today.
Congress also passed the Required Request Law enacted by all 50 states in 1984. This law established consent to organ donation, mandating that hospitals present families of all potential deceased donors with the option of donation.
The 1990s proved successful for many firsts, including the first hand transplant, the first living donor lung transplant, and the first laparoscopic kidney donor surgery. The first kidney-paired donation exchange transplant was also performed.
Twenty-first century transplantation milestones
Policies addressing children’s transplant criteria, the legal basis for kidney-paired donation exchanges, and reimbursement for ancillary expenses incurred by living donors are established. Clinical advancements include the first successful full-face transplant in 2010 and first live birth after uterus transplantation from a deceased donor in 2018. And in 2020, the first Covid-19 patient received a double lung transplant.
The growing field of possibilities in organ and tissue donation continues to improve or save lives. After a slight dip in donors due to the Covid-19 pandemic, donations rebounded, enabling a record-breaking 48,149 organ transplants in 2024, marking a 3.3% increase over 2023 and a 23.3% rise over the previous five years.
Sources
“Organ donation & transplant resources”. United Network for Organ Sharing. https://unos.org/resources/patient/
“Alexis Carrel: Biographical”. The Nobel Prize. https://www.nobelprize.org/prizes/medicine/1912/carrel/biographical/
“Peter Medawar: Biographical”. The Nobel Prize. https://www.nobelprize.org/prizes/medicine/1960/medawar/biographical/
“Organ Donation Legislation and Policy”. Health Resources & Services Administration. https://www.organdonor.gov/about-us/legislation-policy
“Consent to organ donation: a review”. Progress in Transplantation. https://pmc.ncbi.nlm.nih.gov/articles/PMC6776471/
Before Death: Donating Organs or Body
January 12th, 2026This article has been prepared to aid those in considering one of the greatest, life affirming gifts a person can give.
By donating organs or tissue, you could save the lives or ease the suffering of many people. Meanwhile, donating your body for medical education or research contributes to healthcare and scientific advancements that benefit humankind.
What are organ and tissue donations? What organs can I donate? How do you become an organ donor? What organs are in the highest demand? How can you be sure that your wishes for donation will be honored? This article of SevenPonds will attempt to answer your questions.
Things to Know:
- You may elect to donate specific organs and tissue, or your entire body.
- People of all ages can become organ and tissue donors.
- Approximately 750,000 tissue transplants occur annually in the U.S.
- In 2010, approximately 6,500 Americans died waiting for an organ donation transplant.
What kind of organ, tissue, or body donations can I arrange?
Before death, you can donate organs and bone marrow.
After death, you can donate organs, bone marrow, tissue, and your entire body for medical research and education.
To view a list of what specifically you can donate, see our After Death Guide.
Can I become an organ and tissue donor?
Anyone can become a donor regardless of age, race, or medical history, and each case is considered individually after death. Medical history is more important than age; even adults in their 90s have become organ and tissue donors. Don’t rule yourself out. Let the medical professional make the determination at that time.
What organs are commonly donated?
Currently, kidneys, liver, heart, lungs, pancreas, and small intestine are the most common organ donations. According to the United Network for Organ Sharing, over 14,000 Americans become organ donors in 2022, while more than 100,000 Americans are waiting for organ transplants at any given time.
What is tissue?
Tissue is a wide-ranging term for a collection of biological cells, grouped together to carry out a specific function; bone, skin, corneas, tendons and ligaments, cartilage, arteries and veins, and heart valves are all examples of different kinds of tissue. These days, tissue transplantation is a routine part of patient care, and approximately 750,000 tissue transplants occur in the U.S. each year.
How do I arrange for an organ and tissue donation?
Most states, but not all, have donor registries, allowing you to designate yourself as an organ donor when you renew your driver’s license. See the national organ donor website for information on registering in your state.
You should also document your organ and tissue donation preferences in your advance health care directives.
Can I decide what organs or tissue I wish to donate?
Yes. Most states allow you to opt out of donating organs and tissue for medical research and may allow you to opt out of donating specific organs or tissues for transplantation as well. They may also allow you to set additional conditions, such as that your donated tissue may be used only for life-saving or reconstructive purposes or that your organs and tissue can only be distributed in the United States.
If I document my organ and tissue donation preferences, will my wishes be honored?
Each state has specific laws and requirements for organ donation. Even if you obtain an “organ donor” designation on your driver’s license, and state your preferences in advance health care directives, your preferences may still be ignored. For example, your state may also require the consent of the closest relative before organ and tissue donation may proceed. Therefore, it is important to thoroughly research your state’s laws for organ donation and to make certain your family supports your wishes.
Should my family know about my decision?
By all means, discuss your decision to become an organ donor with your family. Make your family aware that none of them will incur the cost of an organ and tissue donation. It is probably wise to designate a relative to serve as your advocate for donation at the time of your death.
How is a potential organ recipient identified?
The United Network for Organ Sharing (UNOS) maintains a national, computerized list of candidates for transplant. Medical compatibility (i.e. tissue type and blood type match), time on the waiting list, medical urgency, and geographic location are used to identify the most suitable donation recipients. For more information on organ donation allocation, see Transplant Living, a website operated by UNOS.
Will organ donation affect my family’s disposition or remembrance event plans?
You can still hold a viewing of a body that has undergone organ donation. The procedure will leave a scar, like any surgery. Your family will still be able to hold a ceremony of their choosing, whether that be a funeral with an open casket, a home funeral, cremation, or natural burial.
How do I donate my body to science?
If you choose to donate your entire body to science or medical research, contact a nearby medical research facility, such as a university medical school. Every facility has different requirements and donation timelines, so you will want to look into this as early as possible. You can also make arrangements to donate your body for medical research and training through a body donation organization.
When planning whole body donation, be sure to discuss any plans you may also have for organ and tissue donation. Often, only one type of donation is accepted at the time of deat,h but in some cases, both may be possible, so if you are interested, be sure to register for both. As with organ and tissue donation, you should document your plans for whole body donation in your advance health care directives, and inform your family of your decision. These steps will help to ensure that your donations are conducted in best accordance with your wishes.
For more information:
Organ, Tissue, & Whole Body Donation: Additional Resources
July 8th, 2025National Organizations
OrganDonor.gov
Managed by the U.S. Department of Health Resources and Service Administration, OrganDonor.gov is the official website of the U.S. government providing information about organ donation to professionals and the public. The website has a great deal of information about the donation process and an interactive map where you can access a form to register as an organ donor in your state.
American Society of Transplantation
Founded in 1982, the American Society of Transplantation is a professional organization made up of transplant physicians, scientists and other healthcare professionals with an interest in transplantation. In addition to supporting research, professional development and advocacy for transplantation, the organization sponsors a community outreach program, which works to educate the public about the importance of funding transplant research and donating organs. You can find answers to many questions about both deceased and living organ donation on its website Power2Save.
Organ Procurement and Transplantation Network
A partnership between the U.S. Department of Health and Human Services and private industry, OPTN is the national network that oversees transplant systems across the U.S. Its board of directors is responsible for setting national policy governing organ and tissue transplantation, following quality metrics, and monitoring areas of concern within the transplant community.It’s website also has an extensive library of resources for patients and members of the community who wish to learn more about the transplant process or how to become an organ or tissue donor.
United Network for Organ Sharing
A nonprofit that operates under contract with the federal government, the United Network for Organ Sharing is a national organization that coordinates transplants across the U.S. The organization is responsible for managing the national transplant waiting list, matching donors to recipients and maintaining a database of all organ transplants that occur in the U.S. The UNOS website has a patient portal where the public can access information about the transplant waiting list, the matching process and more.
Donate Life America
Donate Life America is a nonprofit organization dedicated to increasing the availability of transplantable organs across the U.S. It operates a nationwide education program about the importance of donation and maintains the national Donate Life registry at RegisterMe.org. It’s website also provides an extensive library of information and statistics about organ donation in the U.S.
The American Association of Tissue Banks
The American Association of Tissue Banks is a nonprofit scientific organization that sets standards for the safe use of donated human tissue and provides accreditation for tissue banks throughout the United States. Accredited tissue banks are registered with the FDA and meet AATB standards, which expand on federal regulations around training and competency, safe handling and transport, and on-site safety protocols, including prevention of disease transmission via transplanted tissue. Learn more about tissue donation on the AATB website, or search the AATB database to find an accredited tissue bank in your area.
Science Care
Science Care is a for-profit entity that accepts donated bodies (whole body donation) for use in medical research, education and training across the globe. Donating a body through Science Care is a no-cost option that includes transportation of the deceased to a Science Care affiliate, cremation of the remains after research is complete and return of the deceased’s ashes to the family within about 3-5 weeks. To learn more about the company or to register as a donor call Science Care at (800) 417-3747.
MedCure
Similar to Science Care, MedCure is a for-profit entity that accepts donated whole bodies for use in research and medical education and training. It, too, is a no-cost program for families. The company arranges for transportation of the remains to one of its four U.S. facilities, assumes the cost of cremation, and returns the person’s ashes to the next of kin within about 16 weeks. To learn more about the program or to pre-register as a donor, contact MedCure at 1-866-560-2525 or email donate@medcure.org.
Family & Financial Support
Children’s Transplant Initiative
Children’s Transplant Initiative is a nonprofit that offers peer support and mentorship to children and families undergoing organ transplantation at Texas Medical Center in Houston, Texas. The initiative also helps families with temporary housing and provides direct financial assistance for out-of-pocket expenses associated with the transplant. Use the contact form on the CTI website to learn more.
Help Hope Live
Help Hope Live is a nonprofit fundraising organization that helps patients and families raise money for medical care, including out-of-pocket costs associated with organ transplantation. The organization maintains control over the funds raised and pays bills directly to care providers, so the patients and their families can concentrate on getting well. According to its website, it has helped raise over $135 million for patients in need since its inception in 1986. It has a four-star rating with Charity Navigator, which reports that over 85% of money raised goes to the patients and families it supports.
National Kidney Foundation
The National Kidney Foundation is a nonprofit organization that addresses all aspects of chronic kidney disease, including ongoing research, advocacy, and patient/family support. Founded in 1950, it has been helping those afflicted with chronic kidney disease and those awaiting or undergoing transplant for over 70 years. The NKF offers a number of online support services, including a free information helpline, peer mentoring programs, and online communities for patients undergoing treatment for renal disease. Find these resources and more at the NKF website section Treatment and Support.
American Liver Foundation
The American Liver Foundation is a national research, education and advocacy group that provides resources to the public about liver disease and its treatment, including liver transplantation. Its Phil Scarfo Liver Resource Center offers information on clinical trials, a physician locator, a video library and a number of brochures and educational articles as well as access to online support groups for people living with liver disease. ALF also offers a free telephone helpline Monday through Friday from 9am – 5pm ET at 1-800-465-483, and 24-7 live chat on its website.
Local Organizations
University of California Health
The University of California is a known recipient of whole body donations in the State of California. The UC Anatomical Donation Program is comprised of five of the University of California’s six schools of Medicine at Davis, Irvine, Los Angeles, San Diego and San Francisco. These locations serve as collection and preparation sites for anatomical materials and services that advance scientific research and education among health professionals during residencies. Registration forms can be requested online or downloaded from the UC location nearest you.